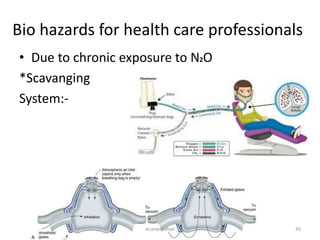
Nitrous oxide inhalation sedation is a commonly used technique for dental procedures in children. It involves administering a mixture of nitrous oxide and oxygen gas through a nasal hood. When properly administered, it can reduce anxiety and pain while allowing the child to remain cooperative. Precise monitoring of vitals and sedation level is important to avoid oversedation. Recovery is typically rapid once nitrous oxide is discontinued and oxygen alone is given. Scavenging systems help protect healthcare workers from exposure during administration.