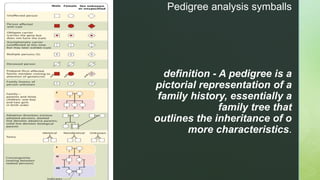
This document discusses pedigree analysis and the different modes of inheritance for genetic traits. It begins by defining a pedigree as a pictorial representation of a family history and inheritance of traits. It then discusses the symbols used in pedigrees to represent generations, individuals, and their characteristics. The document goes on to explain autosomal recessive, autosomal dominant, X-linked recessive, X-linked dominant, and Y-linked traits and provides examples like Tay-Sachs disease, familial hypercholesterolemia, hemophilia, and hypophosphatemia.