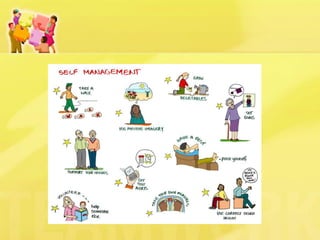
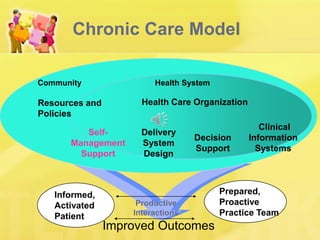
This document discusses patient self-management support, which involves helping patients manage their chronic conditions through education, goal-setting, and developing self-management skills. It describes strategies for supporting self-management, including assessing patient needs and barriers, collaborative goal-setting, enhancing problem-solving skills, and arranging follow-up care. The document also outlines how practices can meet NCQA standards for self-management support and provides resources for implementing self-management programs.
































































![C38 Journey Into Well Being[1]](https://cdn.slidesharecdn.com/ss_thumbnails/c38-journey-into-well-being1-1201798853117630-4-thumbnail.jpg?width=640&height=640&fit=bounds)

















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















