Downloaded 277 times
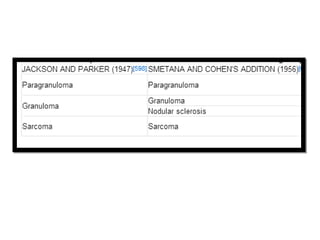
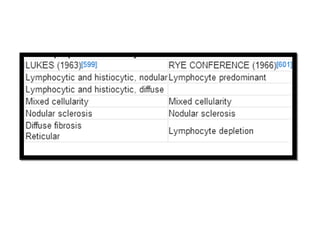
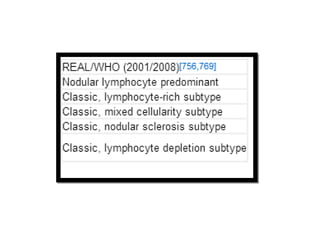
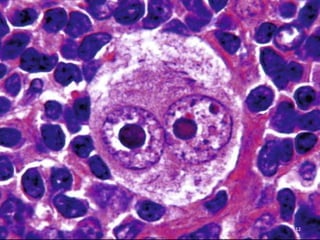
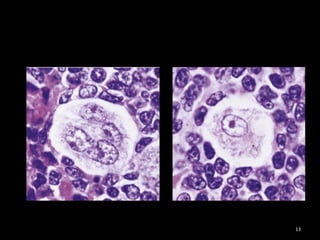
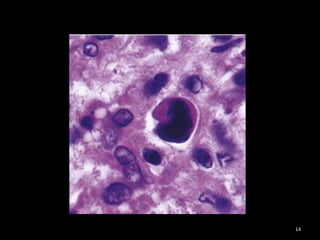

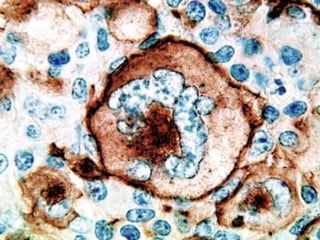
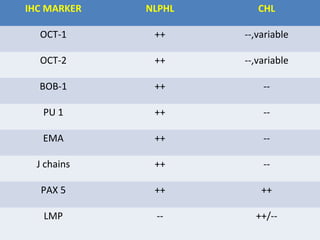
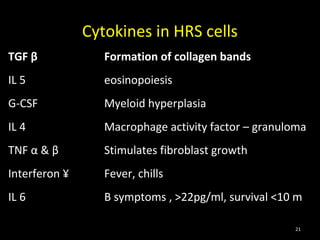

The document summarizes recent advances in Hodgkin's lymphoma. It discusses the history and classification of Hodgkin's lymphoma. It covers immunophenotype markers, involvement of Epstein-Barr virus, genetic changes in Hodgkin-Reed-Sternberg cells, the tumor microenvironment, microRNAs, and mechanisms of chemoresistance. Novel therapies discussed include monoclonal antibodies targeting CD20 and CD30.



































































