This document discusses different types of parenteral fluids used in medical treatment. It covers crystalloids like normal saline and Ringer's lactate, which are preferred due to lower cost and side effects. It also discusses colloids, balanced salt solutions, maintenance fluid volume and type, tonicity versus osmolarity, comparisons of common crystalloid solutions to plasma, and fluids used for resuscitation in dehydration or shock.
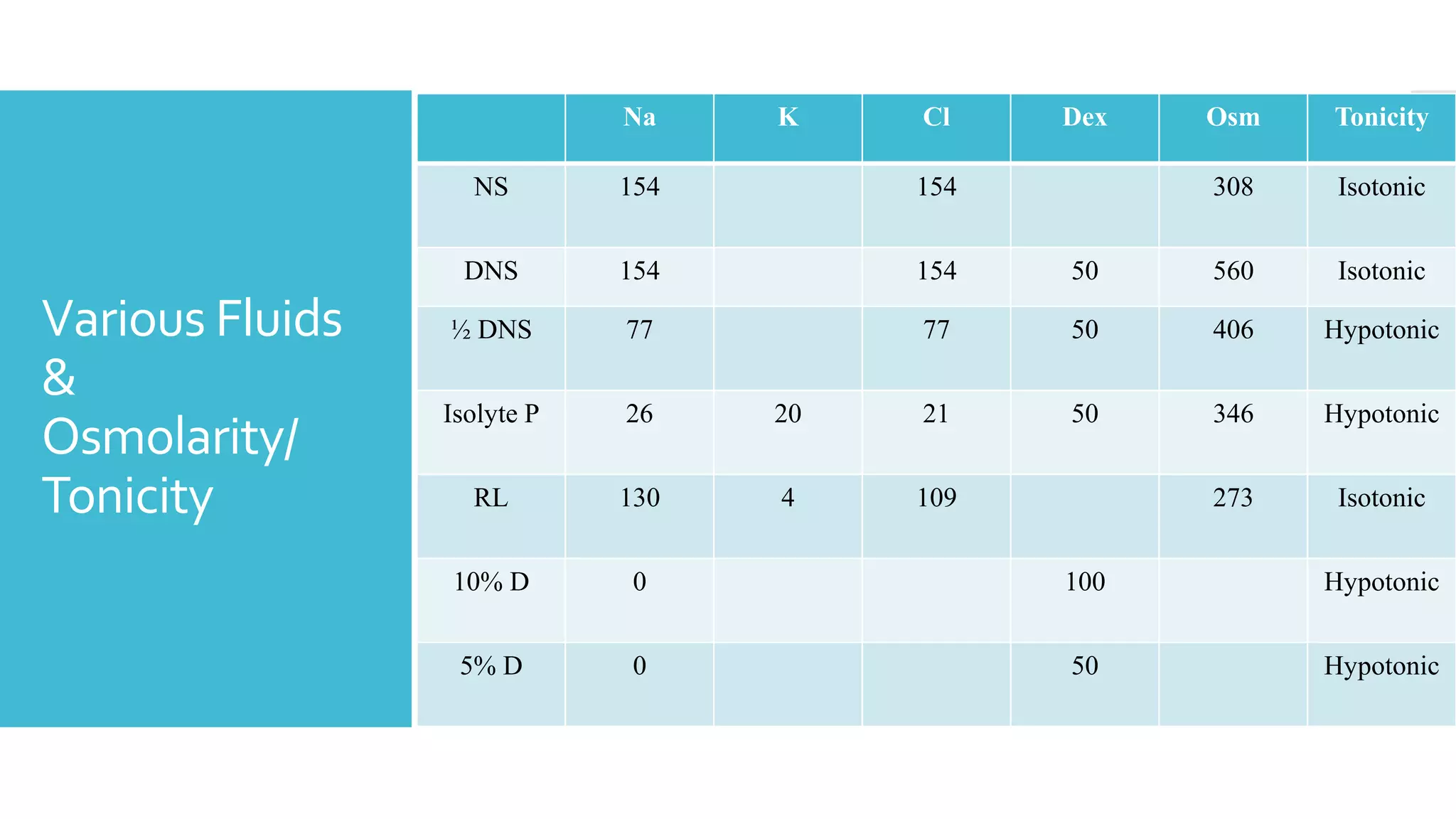
![Tonicity
&
Osmolarity
Osmolarity :
- Number of osmoles of solutes per kg of solution
- Concentration of permeable & impermeable solutes
- 2x[Na] + [glucose]/18+ [BUN]/2.8
Tonicity ( Effective osmolarity ) :
- Concentration of non-permeable solutes
- 2x[Na] + [glucose]/18](https://image.slidesharecdn.com/parenteralfluids-230116193518-77cdfe2a/75/Parenteral-Fluids-pptx-7-2048.jpg)