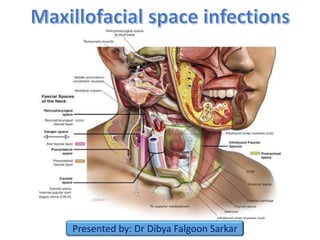
Maxillofacial space infections
•Download as PPTX, PDF•
28 likes•8,132 views

Detailed description of diagnosis and management of maxillofacial and neck space infections. Discussion of anatomy of the spaces is also done in details. Drainage of such spaces are also discussed. Medical management is also discussed. Complications are also discussed.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Maxillofacial space infections
Similar to Maxillofacial space infections (20)
More from Dibya Falgoon Sarkar
More from Dibya Falgoon Sarkar (18)
Recently uploaded
Recently uploaded (20)
Maxillofacial space infections
- 1. Presented by: Dr Dibya Falgoon Sarkar
- 2. Introduction Fascial spaces Fascial layers of Neck Classification of Maxillofacial spaces Stages of infection Microbiology of maxillofacial infections Pathways of spread of dental infection Sequelae of dental infections Diagnosis of maxillofacial space infection Imaging of maxillofacial spaces Antibiotic treatment Surgical management of space infection Discussion of individual space infections
- 3. •The incidence and severity of maxillofacial space infections have diminished since the advent of antibiotic therapy. •However, significant morbidity and mortality of these infections continue. •Dentists and physicians must be alert to the potential seriousness of these infections, which should never be dismissed as simple dental abscesses.
- 4. • Shapiro defined fascial spaces as potential spaces between the layers of fascia. •These spaces are normally filled with loose connective tissues and various structures like veins, arteries, glands, lymph nodes •Space is a misnomer. There are voids in the tissues in actual reality. The term fascia is used to describe broad sheets of dense connective tissues whose function is to separate structures that may pass over each other during movement and serves as pathways for vascular and neural structures.
- 5. Fascial plane Common Name Structures within the Plane Superficial cervical fascia SMAS Platysma, muscles of facial expression Superficial layer of Deep Cervical Fascia (DCF) Investing layer Trapezius, SCM, Anterior belly of digastric, masseter, parotid and submandibular glands Middle layer of DCF Visceral fascia Strap muscles, buccinator, pharyngeal constrictors, esophagus, trachea, thyroid and parathyroid glands Deep layer of DCF Prevertebral fascia Paraspinous muscles, cervical vertebrae, scalene muscles Carotid sheath Confluence of each layer of DCF Common carotid, IJV, Vagus nerve, ansa cervicalis
- 7. Space Anatomy Space 1 Lies superficial to superficial fascia (Subcutaneous space) Space 2 Group of spaces surrounding strap muscles, lying superficial to middle layer of deep cervical fascia Space 3 • Lies superficial to visceral division of middle layer of DCF. • Contains pretracheal, retropharyngeal and lateral pharyngeal spaces Space 3A Carotid sheath (Lincoln’s highway) Space 4 • Potential space between alar and prevertebral division of posterior layer of DCF • Also known as Danger space Space 4A Situated in posterior triangle of neck, posterior to the carotid sheath Space 5 Prevertebral space Space 5A Enclosed by prevertebral fascial, posterior to transverse process pf vertebrae, as it surrounds the scalene and spinal postural muscles
- 9. 1. Direct involvement (Primary spaces) • Maxillary spaces: Canine, buccal, infratemporal • Mandibular spaces: Submental, submandibular, sublingual, buccal 2. Indirect involvement (Secondary spaces) • Masseteric • Superficial and deep temporal • Pterygomandibular • Lateral and retropharyngeal • Prevertebral, parotid, pretracheal, pertonsillar, carotid sheath and danger spaces
- 10. I. Face- Buccal, canine, masticator spaces II. Suprahyoid- Sublingual, submandibular, submental, peritonsillar, lateral pharyngeal III. Infrahyoid- Pretracheal IV.Space of total neck- Retropharyngeal, Danger space, Space of carotid sheath
- 11. Characteristic Inoculation Cellulitis Abscess Duration 0-3 days 3-7 days >5 days Pain Mild- moderate Severe & generalized Moderate-severe & localized Size Small Large Small Localization Diffuse Diffuse Circumscribed Palpation Soft, doughy, mild tender Hard, exquisitely tender Fluctuant, tender Appearance & skin quality Normal Reddened & thickened Peripherally reddened, shiny skin texture Surface temperature Slightly heated Hot Moderately heated Loss of function Minimal Severe Severe Tissue fluid Edema Serosanguinous, flecks of pus Pus Percutaneous bacteria Aerobic Mixed Anaerobic
- 12. 1. Hyperemia and vasodilation 2.Passage of plasma proteins and leukocyte rich exudate into surrounding tissues Precipitation of fibrin network which walls off the affected region 1. Phagocytosis of bacteria and dead cells 2. Disposal of macrophages of necrotic debris Aerobic bacteria Frequency Anaerobic bacteria Frequency Gram- positive cocci (85%) Gram- positive cocci (30%) Streptococcus ( Gr D ,B haemolytic, Viridans) Very common Streptococcus Common Staphylococcus Rare Gram- negative bacilli Gram –ive bacilli (50%) H. Influenzae, E. coli Prevotella, Fusobacterium Very common Eikenella corrodens Porphyromonas Rare
- 14. Periapical infection Bacteremia- septicaemia Deep fascial space infection Ascending cerebral infection Osteomyelitis Intraoral soft tissue abcess Cellulitis Fistula
- 15. Involved teeth Usual exit from bone Relation of muscle to Root apices Site of localization of infection Upper central incisor Labial Oral vestibule Upper lateral incisor Labial Palatal Oral vestibule Palate Upper canine Labial Above (Levator muscle) Below Oral vestibule Canine space Upper premolars Buccal Palatal Above Oral vestibule Palate Upper molars Buccal Palatal Above (Buccinator) Below Oral vestibule Buccal space Palate
- 16. Involved teeth Usual exit from bone Relation of muscle to Root apices Site of localization of infection Lower incisors Labial Above (Mylohyoid) Below Submental space Oral vestibule Lower canine Labial Below (Buccinator) Oral vestibule Lower premolars Buccal Below (Buccinator) Oral vestibule Lower 1st molars Buccal Lingual Below (Buccinator) Above Oral vestibule Buccal space Sublingual space Lower 2nd molars Buccal Lingual Below (Buccinator) Above Below (Mylohyoid) Above Oral vestibule Buccal space Sublingual space Submandibular space Lower 3rd molars Lingual Submandibular/ pterygomandibular space
- 17. • History: 1. Recent dental/ surgical procedures in upper aerodigestive tract 2. Trauma 3. Past medical history: Diabetes, HIV, etc, 4. Drug history • Symptoms: 1. Onset and duration of symptoms 2. Pain, fever, redness at the site, dysphagia 3. Trismus, dyspnoea • Physical examination: 1. Palpation of neck mass, tenderness, crepitation, fluctuance 2. Visual inspection of oral, nasal cavity, oropharynx 3. Upper airway inspection (Flexible fibreoptic illumination) • Laboratory tests: 1. Complete blood count 2. Renal function, blood sugar and hydration status 3. Pus/blood culture and sensitivity
- 18. • Plain films: OPG, A-P/ Lateral cervical radiographs for evaluation of retropharyngeal abscess • CECT scan: Most reliable (95% sensitivity) imaging means for deep neck space infections. • MRI: Helpful when intracranial or neural extension is suspected • MRI useful in patients with impaired renal function • Ultrasonography: Useful for needle drainage and localization. MRI- Cavernous sinus thrombosis CECT scan
- 19. Principles for choosing appropriate antibiotic ( Topazian 4th edition) : 1. Identification of causative organism- Pus, blood or tissue culture 2. Start with empirical therapy till antibiotic sensitivity is obtained 3. Use of a specific, narrow spectrum antibiotic 4. Use the least toxic antibiotic of the sensitivity list 5. Patient’s drug history and medical history should be taken 6. Use of bactericidal rather than bacteriostatic antibiotic 7. Cost of antibiotic 8. Encourage patient compliance 9. Proper dosage and route of administration 10. Combination therapy
- 20. 1. Incise healthy skin and mucosa when possible 2. Place incision in an aesthetically acceptable area 3. Place incision in a dependent area 4. Dissect bluntly and explore every part of abscess cavity up to the infected tooth 5. Place a drain and stabilize it with sutures 6. Consider use of through and through drains in bilateral cases 7. Don’t leave the drains for an extended period of time 8. Clean wound margins daily under sterile conditions Goals of surgical intervention: 1. Providing tissue/ fluids for culture and sensitivity 2. Allowing drainage of pus and irrigation of the isolated infected spaces
- 21. • Boundaries • Anteriorly: Ends at modiolus just posterior to the oral commissure • Posteriorly: Masseter and pterygomandibular raphe • Superiorly: Infraorbital space and anterior surface of maxilla • Inferiorly: Inferior border of mandible • Superficial: Skin ; Deep: Buccinator • Contents: Stensen duct, facial artery and buccal fat pad • Buccal cellulitis: Non odontogenic origin ;Common in children < 3years. Caused by H. influenzae.; high fever for atleast 24 hrs prior clinical signs ; otitis media
- 22. Buccal space Superiorly: Infraorbital space Posteriorly: • Submass- eteric space • Lateral pharyngeal space Medial side: • Pterygo- mandibular space • Infra- temporal space Via buccal fat pad: Superficial temporal space
- 24. • Potential space between oral vestibular mucosa and nearby muscles of facial expression. • Boundaries: • Posteriorly: Buccinator muscle • Anteriorly: Intrinsic muscle of lip like orbicularis oris, etc. • Medially: Alveolus • Contents: Areolar tissue, long buccal and mental nerve • Communicates: buccal and subcutaneous spaces • Drainage: Via buccal vestibule
- 25. • Incidence: Rare • Clinical features: Marked swelling lateral to nose, cellulitis of eyelids and obliteration of nasolabial fold • Boundaries: oSuperiorly: Levator labii superioris & alaque nasi oInferiorly: Caninus muscle oMedially: Anterior surface maxilla, levator anguli oris oAnteriorly: Orbicularis oris, nasal cartilage oPosteriorly: Buccal space, buccinator oMay involve infraorbital space • Drainage: Intraorally high in the maxillary vestibule
- 26. • Boundaries: 1. Anterior: Inferior border of mandible 2. Posterior: Hyoid bone 3. Superior: Mylohyoid muscle 4. Inferior: Investing fascia and skin 5. Lateral: Anterior belly of digastric 6. Superficial: Investing fascia • Likely cause: Lower anteriors, fracture symphysis • Contents: Anterior jugular vein, submental nodes • Communications: Submandibular spaces • Drainage: Extra oral horizontal incision in most inferior portion of chin in a natural skin crease.
- 27. • Boundaries: 1. Anterior: Anterior belly of digastric 2. Posterior: Posterior belly of digastric 3. Superior: Inferior and medial surface of mandible 4. Inferior: Digastric tendon 5. Superficial: Platysma, investing fascia 6. Deep: Mylohyoid, hyoglossus • Likely cause: Lower molars • Contents: Submandibular gland, facial artery and vein, level IB nodes • Communications: Submental, sublingual, lateral pharyngeal, buccal spaces • Drainage: Extraorally by submandibular incision.
- 28. • Stab incision placed below the lower border of mandible over the dependent part • Curved haemostat is passed and blunt dissection is made through subcutaneous fat • Avoid facial artery, vein and marginal mandibular nerve
- 29. • Boundaries: 1. Anteriorly: Inferior border of mandible 2. Posterior: Hyoid bone 3. Superior: Oral mucosa (FOM) 4. Inferior: Mylohyoid muscle 5. Medial: Muscles of tongue 6. Lateral: Lingual surface of mandible • Contents: Sublingual glands, Wharton’s duct, Lingual nerve, sublingual vessels • Likely cause: Lower premolars, first and second lower molar, direct trauma • Communicates: Submandibular, lateral pharyngeal (via buccopharyngeal gap between constrictors) , visceral ( trachea & esophagus)
- 30. Drainage: Incision is placed over floor of mouth in the lingual sulcus parallel to the Wharton’s duct. Lingual nerve and sublingual vessels are preserved.
- 31. • Definition: Firm, acute, toxic cellulitis of the submandibular and sublingual spaces bilaterally and of the submental space. ( Topazian, Goldberg, Hupp ; Oral & Maxillofacial Infections, 4th edition) • Wilhelm von Ludwig first described this condition in 1836 • Cause: Dental infection (90% cases) • Clinical features: Brawny edema over bilateral submandibular region Elevated tongue Airway obstruction Paucity of pus • May spread to masticator spaces
- 32. • Early diagnosis and maintenance of airway • Tracheostomy / fibreoptic laryngoscopy may be considered • Fluid resuscitation • Prolonged, intense, intravenous antibiotic therapy • Use of Inj. Dexamethasone to reduce oedema • Extraction of affected teeth • Early surgical drainage • Incision: Horizontal incision midway between the chin and hyoid bone along with bilateral incisions into the submandibular spaces • Masticator spaces are also drained if trismus is present Signs of airway compromise: 1. Clinical: Dyspnoea, stridor, inability to control secretions 2. Radiographic: Deviation of airway
- 33. • Masticator space is an anatomical compartment enclosed by splitting of the anterior layer of deep cervical fascia around muscles of mastication, following those muscles to their attachments to the cranium and skull base ( Topazian, Goldberg, Hupp ; Oral & Maxillofacial Infections, 4th edition) • Parts: 1. Submasseteric 2. Pterygomandibular 3. Superficial temporal 4. Deep temporal • Common clinical sign: Trismus
- 34. • Boundaries: 1. Superior: Dense attachment of fascia to inferior border of ZM arch 2. Inferior: Pterygomassteric sling 3. Lateral: Masseter 4. Medial: Lateral surface of ramus 5. Anterior: Buccal space 6. Posterior: Parotid gland • Likely cause: Lower 3rd molars, angle of mandible fracture • Contents: Massteric artery and vein • Communications: Pterygomandibular ( Via sigmoid notch), superficial temporal, parotid, buccal spaces • Drainage: Extraorally by submandibular incision near angle of mandible avoiding marginal mandibular nerve
- 35. Superficial temporal space • Boundaries: 1. Anterior: Posterior surface of lateral orbital rim 2. Posterior: Fusion of temporal fascia to cranium 3. Superior: Superficial temporal crest 4. Inferior: ZM arch and submassteric space 5. Lateral: Temporal fascia 6. Medial: Temporalis muscle • Likely cause: Upper and lower molars • Contents: Temporal fat, temporal branch of VII nv • Communications: Deep temporal, buccal spaces • Drainage: a. Percutaneously by incision superior and parallel to ZM arch b. Intraorally: Sicher’s incision ( Not possible in trismus)
- 36. • Boundaries: 1. Anterior: Posterior surface of maxilla, 2. Posterior: Temporalis attachment to crest 3. Superior: Temporal crest 4. Inferior: Superior surface of lateral pterygoid 5. Lateral: Temporalis muscle 6. Medial: Squamous temporal bone, sphenoid • Likely cause: Upper molars • Contents: Pterygoid plexus, internal maxillary vessels, mandibular nerve, skull base foramina • Communications: Superficial temporal,inferior petrosal sinus, buccal • Drainage: Intraorally via Sicher’s incision
- 37. • Boundaries: 1. Anterior: Buccal space 2. Posterior: Parotid gland 3. Superior: Lateral pterygoid, infratemporal space 4. Inferior: Inferior border of mandible 5. Lateral: Ascending ramus 6. Medial: Medial pterygoid • Likely cause: Lower 3rd molars, angle of mandible fracture • Contents: Inferior alveolar nerve and vessels • Communications: Deep temporal, submassteric, lateral pharyngeal, parotid, buccal spaces • Drainage: Extraorally by submandibular incision near angle of mandible avoiding marginal mandibular nerve
- 38. • Formed by splitting of the anterior layer of deep cervical fascia to form capsule of parotid gland. • Parotideomasseteric fascia is thick laterally and thin medially. • Content: Parotid gland, branches of facial nerve, posterior facial vein • Clinical features: Very painful since the overlying fascia is tenacious. • Drainage: Preauricular modified Blair incision
- 40. • Boundaries: 1. Anterior: Palatal musculature (sup.),superior and middle constrictor muscle, stylohyoid (inf.) 2. Posterior: Carotid sheath and scalene fascia 3. Superior: Skull base 4. Inferior: Hyoid bone 5. Lateral: Medial pterygoid muscle 6. Medial: Pharyngeal constrictor, bucco- pharyngeal fascia, retropharyngeal space • Likely cause: Lower 3rd molars, tonsils, infections in neighbouring spaces • Contents: Carotid artery, IJV, vagus nerve, sympathetic chain • Communications: Submandibular, sublingual, peritonsillar, retropharyngeal spaces
- 41. Inverted pyramid shaped with apex at hyoid bone. Space is divided into 2 compartments : (by Aponeurosis of Zuckerkandl & Testut) 1. Anterior (prestyloid) - Areolar tissue 2. Posterior (poststyloid) – Cranial nerves IX- XII, Carotid sheath and its contents Clinical signs: • Airway obstruction and dysphagia in severe cases • Visible swelling in suprahyoid region between posterior belly of digastric and anterior border of SCM • Intraorally mild trismus, blunted ipsilateral palatoglossal arch, deviated uvula. • Imaging : CECT of neck Church- steeple sign
- 43. • Therapy consists of antibiotics, surgical drainage, tracheostomy if indicated. • Incisions: 1. Oral: Vertical incision on lateral pharyngeal wall over PTM raphe. Blunt dissection made lateral to superior constrictor. 2. Extraoral: • Incision made along anterior border of SCM extending from below angle of mandible • Exposure of the carotid sheath near the lateral tip of hyoid by retracting the SCM posteriorly. • Blunt dissection along posterior border of digastric muscle leads to lateral pharyngeal space 3. Combined intra and extraoral approach
- 44. • Boundaries: 1. Anterior: superior and middle constrictor muscle 2. Posterior: Alar fascia 3. Superior: Skull base 4. Inferior: Fusion of alar with prevertebral fascia at C6-T4 5. Lateral: Carotid sheath and lateral pharyngeal space • Likely cause: Nasal and pharyngeal infections in children, dental infections, esophageal trauma/ foreign bodies and tuberculosis. • Contents: Retropharyngeal nodes • Communications: Submandibular, sublingual, peritonsillar, lateral pharyngeal spaces
- 45. • Clinical features: 1. Dysphagia, dyspnoea 2. Fever , nuchal rigidity 3. Oesophageal regurgitation 4. Buldging of posterior pharynx 5. Risk of rupture of pharyngeal wall during intubation • Radiographs: 1. Lateral soft tissue radiographs: Widening of the space ( Normal width: Adults- 3-6mm, Children- >14mm at C2 level) 2. CT scans: Loss of curvature of cervical spine • 10-40% infections resolve with medicines • Drainage: 1. Trans orally - Under local anaesthesia in Trendelenburg position with constant suctioning. Incision made through posterior wall of pharynx. 2. External approach - • More dependent drainage, deep drains are placed. • Incision made along ant. border of SCM and parallel to it, inferior to hyoid bone • Avoid injuring XII nerve and carotid sheath while blunt dissection 3. Needle aspiration of the abscess under CT guidance
- 46. • Named due to its communication with posterior mediastinum • Relations: 1. Above: Skull base 2. Below: Diaphragm 3. Lateral extent is at fusion of alar and prevertebral fascia at the transverse process of cervical and thoracic vertebrae. 4. Midline structure behind retro- pharyngeal space. • According to Pearse et al study on 110 cases of mediastinitis: a) 71% cases- From danger space b) 21% cases- From carotid sheath c) 8% cases- From pretracheal space
- 47. Complication Notes Symptoms & Signs Diagnosis & Management Cavernous sinus thrombosis • Often direct spread of Streptococcus/ Staphylococcus from paranasal sinuses • Mortality- 30-40% Picket fence fever, orbital pain, proptosis, decreased ocular motility, sluggish pupillary reflex, dilated pupil, loss of consciousness MRI with contrast ICU care Broad spectrum antibiotics Anticoagulation Mediastinitis Caused due to descending infection via danger space and carotid sheath Mortality- 30-40% Diffuse neck edema Dyspnea Mediastinal widening Pleuritic chest pain Hypoxia, tachycardia o CT with contrast o Broad spectrum antbiotics o Transcervical/ transthoracic drainage Necrotizing fascitis Often caused due to odontogenic infection in immunocomp- romised patient Does not follow fascial planes o Rapidly progressive cellutis o Pitting edema, painful o Subcutaneous crepitus • CT with contrast demonstrating tissue gas, necrosis • ICU care, resuscitation • Debridements • Hyperbaric oxygen • Treatment of underlying condition Lemierre syndrome • Fusobacterium necrophorum • Potentially fatal Fever, sore throat Trismus Lateral neck tenderness, septic emboli CT with contrast showing IJV thrombosis Beta lactamase antibiotics +/- surgery
Editor's Notes
- CECT scan: Discrete low attenuation areas within soft tissue inflammatory mass with an enhancing peripheral rim MRI > CT scan in demonstrating bone marrow alterations
- We should always keep in mind about fluid resuscitation during drainage
- Occupies the space between the facial skin and buccinator muscle Recurrent buccal cellulitis : Crohn’s disease
- Likely causes: Upper and lower premolars, upper molars
- Stab incision placed below the lower border of mandible with No. 11 BP blade
- When infections perforate the alveolus below the origin of buccinator Dentoalveolar abcesses occupy some portion of vestibular space
- When maxillary canine infection perforates the maxillary buccal cortex superior to origin of levator muscle of upper lip
- Also known as submaxillary space Clinical signs: Submandibular swelling
- Clinical signs: Elevation of tongue, pus collects just behind the epiglottis which makes intubation difficult
- D/D: Submassteric swelling obscure ear lobe ; parotid swellings elevate ear lobe
- Sicher’s incision: Intraorally vertical incision is made medial to the anterior border of the mandibular ramus. Haemostat is passed superiorly along the lateral aspect of the coronoid process into the superficial temporal space
- Sicher’s incision: Intraorally vertical incision is made medial to the anterior border of the mandibular ramus. Exception: Haemostat is passed supero-medially along the medial aspect of coronoid process to enter the DT space
- Cause : Needle track infections during IANB CT scan: Edematous pterygoid muscle; deviation of uvula to opposite side clinically Intraoral drainage: Not possible in trismus If no trismus: Intraoral incision in mucosa between medial aspect of ramus and the PTM raphe