Download as PDF, PPTX




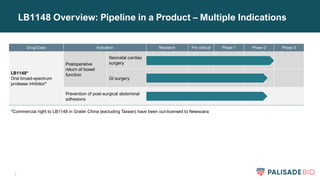
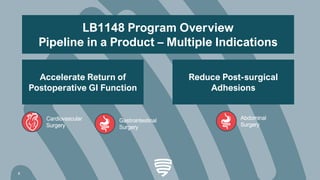
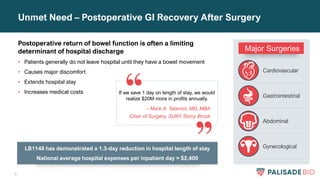
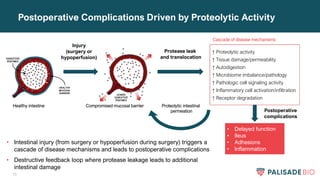
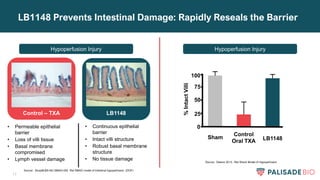
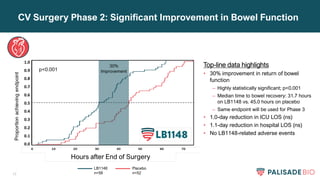
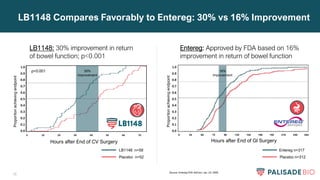
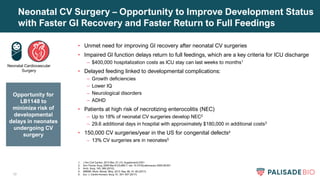
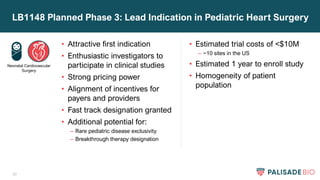
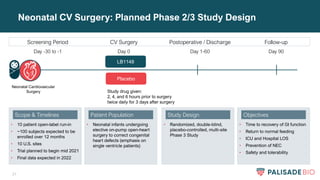
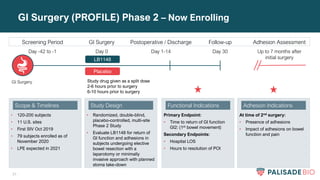

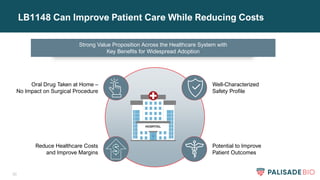




- Palisade Bio was formed through the merger of Leading BioSciences and Seneca to focus on developing drugs to restore intestinal barrier health. - Their lead product, LB1148, is an oral protease inhibitor that has shown in clinical trials to accelerate the return of normal bowel function after surgery by 30%. - They plan to initiate a Phase 3 trial in 2021 to evaluate LB1148 in improving GI recovery in neonates undergoing cardiac surgery, which could potentially qualify for priority review. - If successful, LB1148 has the potential to reduce postoperative complications and lower healthcare costs through shorter hospital stays.