Downloaded 15 times


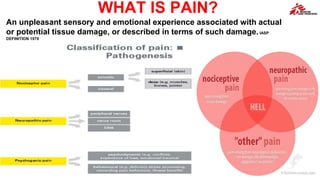

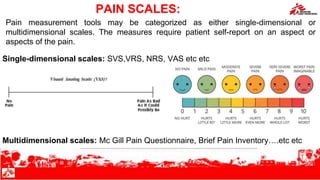
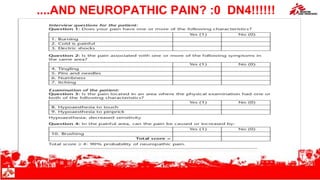



The document outlines an overview of pain management content, covering types of pain, assessment methods, and treatment protocols. It emphasizes the importance of accurate pain evaluation using various scales and recommends timely administration of analgesics based on pain intensity. Additionally, it addresses the management of neuropathic pain through multimodal treatment approaches, highlighting self-reporting as the most reliable indicator of pain.















































































