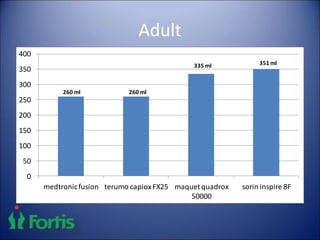
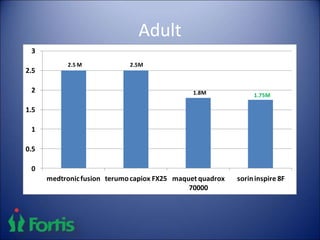
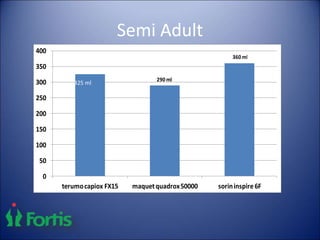
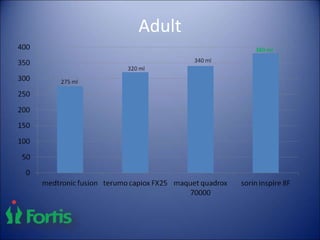
1) Choice of oxygenator depends on factors like priming volume, membrane surface area, blood flow rates, and microemboli production. Lesser priming volumes and surface areas are preferred to reduce hemodilution and cell trauma.
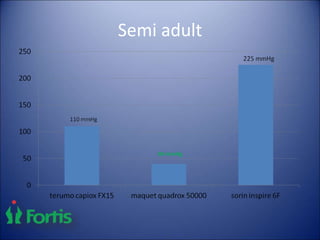
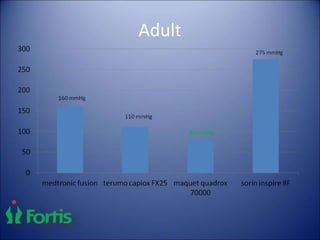
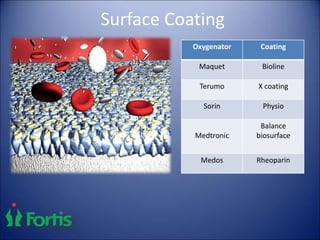
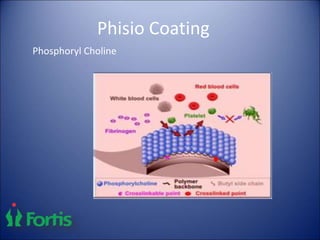
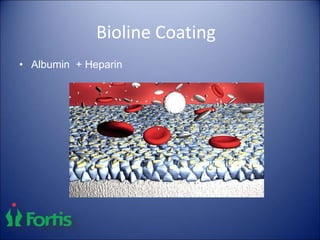
2) Features of an ideal oxygenator include low priming volume, compact design, high maximum flow rates, minimal pressure drop, and effective management of gaseous microemboli. Surface coatings like phosphoryl choline and albumin aim to reduce inflammation.
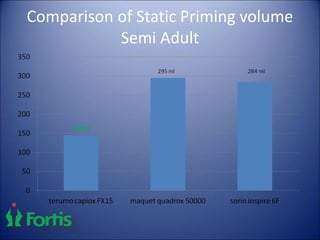
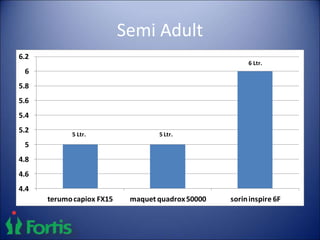
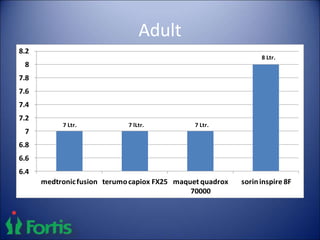
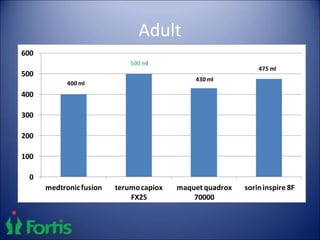
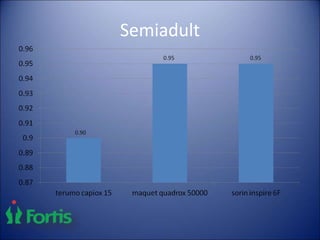
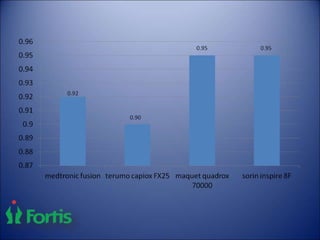
3) For adults, the Sorin Inspire 8F, Maquet Quadrox 70000, and Terumo RX25 are recommended oxygenators based on their specifications and performance.