By the endof this session you should be
By the end of this session you should be
able to describe:
able to describe:
What is a fracture?
What is a fracture?
Types of fractures..
Types of fractures..
Causes..
Causes..
Clinical Features..
Clinical Features..
Healing of fractures..
Healing of fractures..
Complications..
Complications..
Principles of management..
Principles of management..
4.
Definition
“Loss of continuityin the substance of a
bone is called a fracture.”
Spectrum extends from a microscopic
fracture to a hair line fracture and than to
grossly notable fractures.
Types (cont,d)
Avulsionfracture:
Muscle or ligament pulls on a bone fracturing it.
Comminuted fracture:
Bone is shattered into many pieces
Compression fracture:
Collapse of bone usually vertebra in osteoporosis
Fracture dislocation:
Greenstick fracture:
One side of bone fractures, not complete and bone bends
Hair line fracture:
Impacted fracture:
Fragments of bone got impacted
Intraarticular fracture:
7.
Types (cont,d)
Longitudinalfracture:
Along the length of bone
Oblique fracture:
Fracture is diagonal to bones long axis
Pathological fracture:
Spiral fracture:
Atleast one part of bone has twisted
Stress fracture:
Bone breaks because of repeated stresses and strains e.g. athletes
Transverse fracture:
A straight break right across a bone
8.
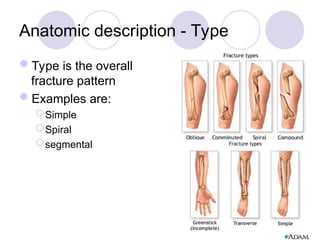
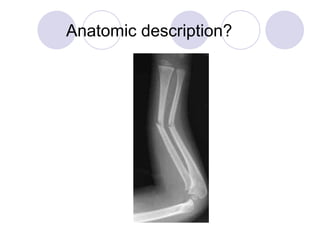
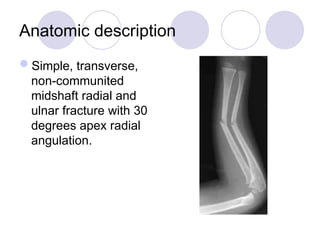
Anatomic description -Type
Type is the overall
fracture pattern
Examples are:
Simple
Spiral
segmental
Anatomic description -Comminution
Comminution is the measure of the
number of pieces of broken bone that
there are.
Examples are: non-comminuted or mildly
comminuted or severely comminuted
11.
Anatomic description -Location
Location is the anatomic location of the
fracture usually described by giving the
bone involved and location on the bone
Examples are: distal radial shaft, proximal
1/3 humeral shaft, intra-articular distal
tibial
12.
Anatomic description -Displacement
Displacement is the amount the pieces of
a fracture have moved from their normal
location
Can be displaced or non-displaced
Subdivided into 3 sub-categories:
translation, angulation, and shortening
13.
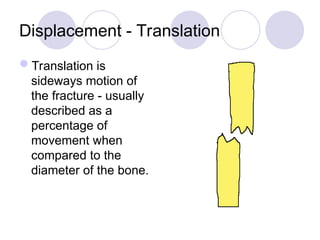
Displacement - Translation
Translationis
sideways motion of
the fracture - usually
described as a
percentage of
movement when
compared to the
diameter of the bone.
14.
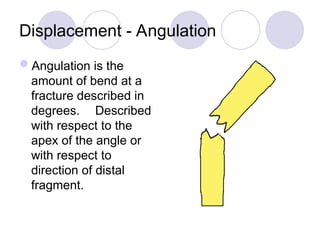
Displacement - Angulation
Angulationis the
amount of bend at a
fracture described in
degrees. Described
with respect to the
apex of the angle or
with respect to
direction of distal
fragment.
Types of classifications
Anatomicdescription
AO classification for Long bone fracture
( Humerus, Radius/ Ulna, Femur, Tibia/
Fibula)
Salter-Harris classification for Epiphysial
plate fracture
Gustillo anderson classification for
open fracture
AO Classification
1st
number =long bone
2nd
number = bone segment
Letter = fracture type (A,B,C)
Then 3rd
& 4th
numbers classify fracture group
& subgroup
22.
Oblique fracture ProximalFemoral Shaft :
(32 A2.1)
3 … the bone … femur
(1= Humerus, 2= Radius/ Ulna, 3= Femur, 4= Tibia/
Fibula)
2 … the segment … diaphysis
(1= Epiphysis, 2= Diaphysis, 3= Metaphysis)
A … the type … least severe
(A= least severe, B= Intermediate, C= Most severe)
2 … the group … Gp. 2 includes oblique fractures
1 … the subgroup … 1 includes fracture in proximal
part of diaphysis
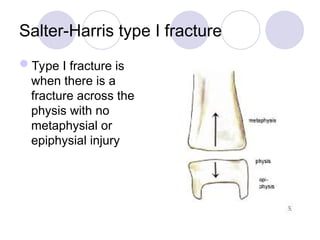
Salter-Harris type Ifracture
Type I fracture is
when there is a
fracture across the
physis with no
metaphysial or
epiphysial injury
25.
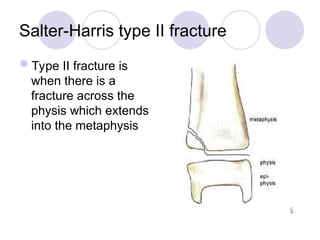
Salter-Harris type IIfracture
Type II fracture is
when there is a
fracture across the
physis which extends
into the metaphysis
26.
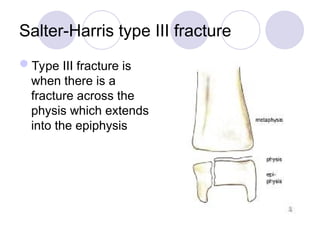
Salter-Harris type IIIfracture
Type III fracture is
when there is a
fracture across the
physis which extends
into the epiphysis
27.
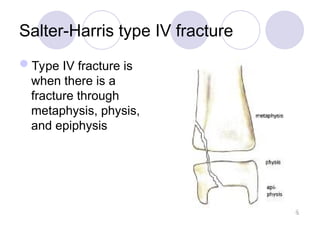
Salter-Harris type IVfracture
Type IV fracture is
when there is a
fracture through
metaphysis, physis,
and epiphysis
28.
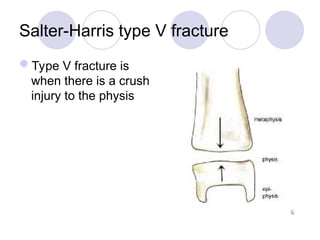
Salter-Harris type Vfracture
Type V fracture is
when there is a crush
injury to the physis
29.
Gustillo classification
The Gustilloclassification is used to
classify open fracture - ones in which the
skin has been disrupted
Three grades that try to quantify the
amount of soft tissue damage associated
with the fracture
30.
Open fractures -grade 1
wound less than 1 cm with minimal soft
tissue injury
wound bed is clean
bone injury is simple with minimal
comminution
With IM nailing, average time to union
is 21-28 weeks
31.
Open fractures -grade 2
wound is greater than 1 cm with
moderate soft tissue injury
wound bed is moderately contaminated
fracture contains moderate
comminution
With IM nailing, average time to union
is 26-28 weeks
32.
Open fractures -grade 3A
wound greater than 10 cm with
crushed tissue and contamination
soft tissue coverage of bone is usually
possible
With IM nailing, average time to union
is 30-35 weeks
33.
Open fractures -grade 3B
wound greater than 10 cm with
crushed tissue and contamination
soft tissue is inadequate and requires
regional or free flap
with IM nailing, average time to union
is 30-35 weeks
34.
Open fractures -grade 3C
is fracture in which there is a major
vascular injury requiring repair for limb
salvage
in some cases it will be necessary to
consider BKA following tibial fracture
Clinical Features
Dependswhich bone affected, patients age, general health, severity
of injury.
Pain
Swelling
Bruising
Discoloured area around affected area
Angulation
Inabbility to bear weight
Inability to move/ painful active or passive movements
Grating sensation/ crepitus
Bleeding if open fractures
If large bone leading to occult bleeding … pallor and dizziness,
feeling of sickness & nausea
37.
Healing of Fractures
Properalignment & immobility, healing is
straightforward
Osteoclasts absorbs old & damaged bone
Osteoblasts create new bone
Callus is new bone formed around
fracture site
38.
Setting a Break
Boneis constantly in a state of turnover, even
Bone is constantly in a state of turnover, even
when not damaged or injured.
when not damaged or injured.
In order for the fracture to heal without any
In order for the fracture to heal without any
deformity, a good ‘reduction,’ or placement, of
deformity, a good ‘reduction,’ or placement, of
the bones must be attained.
the bones must be attained.
If the reduction cannot be satisfactorily
If the reduction cannot be satisfactorily
achieved then a further procedure may be
achieved then a further procedure may be
necessary, such as an
necessary, such as an operation with fixation
with fixation
of the bone with plates, screws or nails.
of the bone with plates, screws or nails.
39.
Factors affecting healingprocess
Patient,s age
Bone affected
Type of fracture
Patient general health condition
Smokers
40.
Complications in FractureHealing
Heals in wrong position
Known as Malunion … either heals in wrong position
or fracture shifts
Disruption of bone growth
If fracture affects growth plate, subsequent deformity
Persistent bone or bone marrow infection
If break in skin … can lead to chronic osteomyelitis
Bone death (Avascular necrosis)
If bone loses its essential blood supply
41.
Principles of GeneralFracture
Management (REST)
Rest
Elevation
Support & Immobilization:
Bones are aligned in anatomical position &
must stay align during process of healing.
Temperature (warmth)
Definition:
Open Reduction InternalFixation.
Open reduction internal fixation is a method of surgically repairing a fractured bone.
Generally, this involves either the use of plates and screws or an intramedullary (IM) rod to stabilize the bone.
O.R.I.F.
O.R.I.F.
44.
Definition:
Definition: Intra medullarynails or
Intra medullary nails or
rods are devices used to stabilize
rods are devices used to stabilize
fractures and allow for bone healing.
fractures and allow for bone healing.
IM nails are inserted into the
IM nails are inserted into the
medullary (bone marrow) canal in the
medullary (bone marrow) canal in the
center of the long bones of the
center of the long bones of the
extremities (e.g. femur, tibia, etc.).
extremities (e.g. femur, tibia, etc.).
Intra medullary Rods
Intra medullary Rods








































![Lecture 25 Intermuscular sapces and axilla [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lecture25intermuscularsapcesandaxillaautosaved-251110002658-47b36c78-thumbnail.jpg?width=640&height=640&fit=bounds)




























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)