1
Presented by
Aparajita
Tiwari
Pg Istyr
Ulcerative & Vesiculo Bullous
Disorders
Guided by
Dr Archana Sudheer
Dr Amit Kumar Singh
Dr Anjali Kumari
Dr Kumar Anand
Dr Susmit Sneha
4
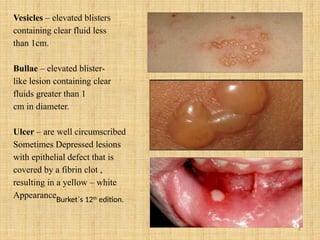
Vesicles – elevatedblisters
containing clear fluid less
than 1cm.
Bullae – elevated blister-
like lesion containing clear
fluids greater than 1
cm in diameter.
Ulcer – are well circumscribed
Sometimes Depressed lesions
with epithelial defect that is
covered by a fibrin clot ,
resulting in a yellow – white
Appearance.
Burket`s 12th
edition.
7
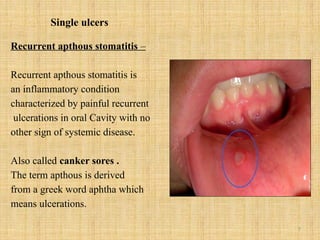
Single ulcers
Recurrent apthousstomatitis –
Recurrent apthous stomatitis is
an inflammatory condition
characterized by painful recurrent
ulcerations in oral Cavity with no
other sign of systemic disease.
Also called canker sores .
The term apthous is derived
from a greek word aphtha which
means ulcerations.
10
Pathogenesis –
Lymphocyte infiltrationin the epithelium causing
erythema ( preulcerative stage)
Followed by localised papule
Surrounded by a reactive erythematous halo due to inflammatory
reaction.
The painful papule then ulcerates(ulcerative phase)
A pseudo membrane covers the ulcer , which is infiltrated mainly
by neutrophils, lymphocytes and plasma cells.
Finally there is healing with epithelial regeneration. (healing
phase)
11.
11
Classification based onthe nature of recurrence
• Simple apthous
• Complex apthous
• Recurrence occurs 2-4 times
a year.
• The disease activity is
almost continuous
throughout the year with
newer lesions developing as
older lesions heal , usually
• Complex apthosis is
associated with systemic
diseases.
12.
12
Classification based onthe frequency of reccurence
Type A
• Type B
• Type C
• RAS episodes lasting a few
days with tolerable pain and
few occurences a year.
• Painful RAS lasting 3-10
days with reccurence every
month.
• Chronic painful course with
disease activity almost
continous throughout the
year.
13.
13
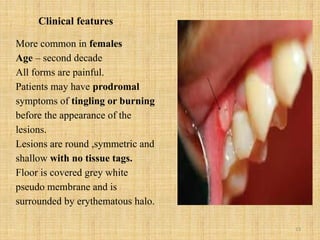
Clinical features
More commonin females
Age – second decade
All forms are painful.
Patients may have prodromal
symptoms of tingling or burning
before the appearance of the
lesions.
Lesions are round ,symmetric and
shallow with no tissue tags.
Floor is covered grey white
pseudo membrane and is
surrounded by erythematous halo.
14.
14
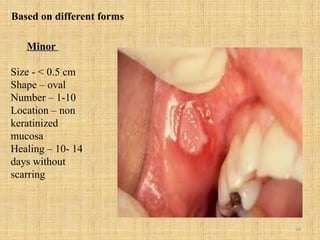
Minor
Size - <0.5 cm
Shape – oval
Number – 1-10
Location – non
keratinized
mucosa
Healing – 10- 14
days without
scarring
Based on different forms
19
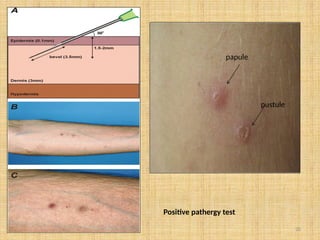
Investigations-
• Serum estimationof vit B12 , Iron & other nutritional deficiency.
• Complete blood count
• Cytosmear/exfoliative cytology
• Pathergy test to rule out behcet`s syndrome.
• Pathergy test - pathergy phenomenon is the state of altered tissue
reactivity that occurs in response to minor trauma.
• Skin/mucosal injury caused by needle prick induces an
inflammatory response.
• Bluntsd needle is introduced into the dermis making four needle
pricks near to each other at an angle of approx 30 degree such that
3-4 mm of needle is buried within the skin .
• Papule seen in atleast 2 needle insertion
• Pustule seen in atleast 1 needle insertion.
21
Treatment
Minor form –first time with very few recurrences
avoidance of stimulus like stress
Avoidance of food that are hard , salty , spicy, acidic
Treatment of anemia if present.
Local analgesics 3-4 application topical
Tablet vit B12 with folic acid twice daily for 7 days
Antiseptic mouthwash ( benzydamine hydrochloride) 3-4 times a
Day.
Topical application of drugs like Amlexanox apply 3-4 times a
day .
22.
22
Treatment
Minor form –if ulcers are occuring very frequently
topical steroids 3-4 times a day ( clobetasol ointment 0.05%,
triamcinolone acetonide 0.1% apply 3-4 times a day).
Intralesional steroids ( 10- 20 mg insoluble triamcinolone
acetonide or 2 mL dexamethasone in dilution with 0.5 mL
saline or 2% lidocaine injected to lesion …..injected directly
into the lesion 3-4 times /week or two times / week .
23.
23
Treatment
Major form –
Intralesionalsteroids
Combination of topical and systemic steroid
( prednisolone 40- 60 mg / day for 5 days)
Immunomodulatory drugs –
Levimasole – 150 mg bid for 5 days
Dapsone – 100 mg / day for 5 days
Azathioprine – 50 mg / day for 5 days
24.
24
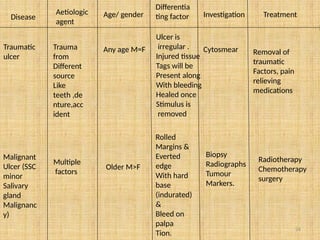
Disease
Aetiologic
agent
Age/ gender
Differentia
ting factorInvestigation Treatment
Traumatic
ulcer
Trauma
from
Different
source
Like
teeth ,de
nture,acc
ident
Any age M=F
Ulcer is
irregular .
Injured tissue
Tags will be
Present along
With bleeding
Healed once
Stimulus is
removed
Cytosmear Removal of
traumatic
Factors, pain
relieving
medications
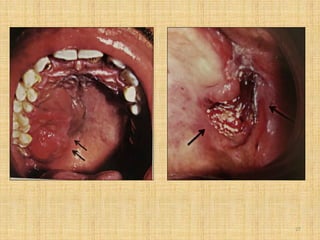
Malignant
Ulcer (SSC
minor
Salivary
gland
Malignanc
y)
Multiple
factors
Older M>F
Rolled
Margins &
Everted
edge
With hard
base
(indurated)
&
Bleed on
palpa
Tion.
Biopsy
Radiographs
Tumour
Markers.
Radiotherapy
Chemotherapy
surgery
26
Disease
Aetiologic
agent
Age/
gender
Differentiating
factor
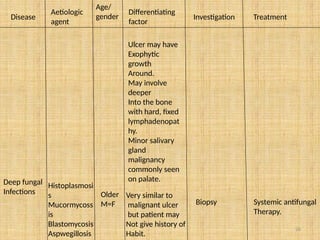
Investigation Treatment
Ulcer mayhave
Exophytic
growth
Around.
May involve
deeper
Into the bone
with hard, fixed
lymphadenopat
hy.
Minor salivary
gland
malignancy
commonly seen
on palate.
Deep fungal
Infections
Histoplasmosi
s
Mucormycoss
is
Blastomycosis
Aspwegillosis
Older
M=F
Very similar to
malignant ulcer
but patient may
Not give history of
Habit.
Biopsy Systemic antifungal
Therapy.
28
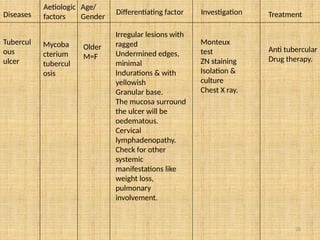
Diseases
Aetiologic
factors
Age/
Gender
Differentiating factor InvestigationTreatment
Tubercul
ous
ulcer
Mycoba
cterium
tubercul
osis
Older
M=F
Irregular lesions with
ragged
Undermined edges,
minimal
Indurations & with
yellowish
Granular base.
The mucosa surround
the ulcer will be
oedematous.
Cervical
lymphadenopathy.
Check for other
systemic
manifestations like
weight loss,
pulmonary
involvement.
Monteux
test
ZN staining
Isolation &
culture
Chest X ray.
Anti tubercular
Drug therapy.
30
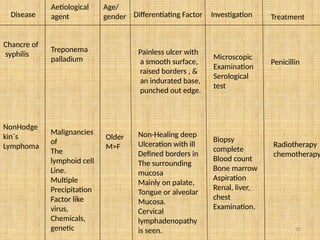
Disease
Aetiological
agent
Age/
gender Differentiating FactorInvestigation Treatment
Chancre of
syphilis
Treponema
palladium
Painless ulcer with
a smooth surface,
raised borders , &
an indurated base,
punched out edge.
Microscopic
Examination
Serological
test
Penicillin
NonHodge
kin`s
Lymphoma
Malignancies
of
The
lymphoid cell
Line.
Multiple
Precipitation
Factor like
virus,
Chemicals,
genetic
Older
M>F
Non-Healing deep
Ulceration with ill
Defined borders in
The surrounding
mucosa
Mainly on palate,
Tongue or alveolar
Mucosa.
Cervical
lymphadenopathy
is seen.
Biopsy
complete
Blood count
Bone marrow
Aspiration
Renal, liver,
chest
Examination.
Radiotherapy
chemotherapy
32
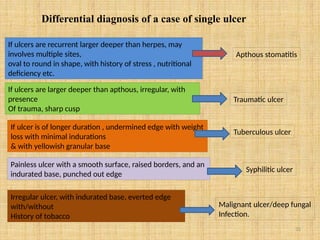
Differential diagnosis ofa case of single ulcer
If ulcers are recurrent larger deeper than herpes, may
involves multiple sites,
oval to round in shape, with history of stress , nutritional
deficiency etc.
Apthous stomatitis
If ulcers are larger deeper than apthous, irregular, with
presence
Of trauma, sharp cusp
Traumatic ulcer
If ulcer is of longer duration , undermined edge with weight
loss with minimal indurations
& with yellowish granular base
Tuberculous ulcer
Painless ulcer with a smooth surface, raised borders, and an
indurated base, punched out edge
Syphilitic ulcer
Irregular ulcer, with indurated base, everted edge
with/without
History of tobacco
Malignant ulcer/deep fungal
Infection.
33.
33
Multiple ulcers –having history of vesicles & bulla
Herpes simplex infection/ acute herpetic gingivostomatitis –
Belongs to herpes viridae family , is a double stranded DNA virus.
Caused by HSV1 ( oral & pharyngeal infection)
HSV 2 ( genital infections)
Primary herpetic stomatitis
Recurrent herpetic stomatitis/
secondary herpetic stomatitis
/herpis labialis
34.
34
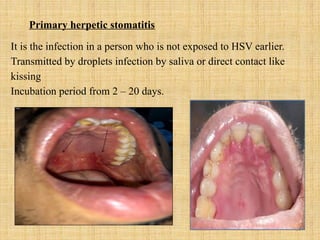
Primary herpetic stomatitis
Itis the infection in a person who is not exposed to HSV earlier.
Transmitted by droplets infection by saliva or direct contact like
kissing
Incubation period from 2 – 20 days.
35.
35
Pathway of HSVinfection
• Primary Herpes simplex is the herpes infection in a person who
is not exposed to this earlier.
• Following infection and local replication at mucosal surfaces,
HSV 1 enters sensory nerve endings and is then transported to
the nerve ganglia.
The virus reaches nerve ganglia ( trigeminal for HSV1 ,
lumbosacral for HSV2 ) & remains latent there until reactivated.
36.
36
Presence of prodromalfeatures fever , irritability, headache, pain
upon swallowing,Regional lymphadenopathy
Within few days mouth becomes painful & the gingiva becomes inflamed
Formation of multiple vesicles, which are clustered together
Vesicles ruptured to form shallow ulcers surrounded by an erythematous halo
On gingiva this lesion presents as multiple small ulcer seen as acute marginal gingivitis
They heal spontaneously within 7-14 days and leave no scar
37.
37
Differential diagnosis
If ulcersite not specific
• Apthous ulcer
• Pemphigus
• Pemphigoid
• Erythema multiforme
If lesion confined only to gingiva
• Erosive/ atrophic LP
• Pemphigus
• Pemphigoid
• ANUG
38.
38
Investigations
• Cytosmear/exfoliative
cytology
• Isolation& tissue culture
• Scrappings of lesion , stain
with Wright`s, giemsa stain,
PAP stain
• Demonstrates balloon cells,
multinucleated giant cells &
intranuclear inclusions
bodies.
• Isolation of virus in tissue
culture, by DNA scappings
from lesions.
39.
39
Investigation
• Detection ofviral DNA
• Antibody titres/
serological methods
• Most sensitive &
accurate method is PCR
technique.
• Detection of antibody
against herpes.
40.
40
Treatment
To relieve pain
Tomaintain
proper fluid
Balance
Mild – moderate
cases
Analgesics topical / systemic
Diphenhydramine hydrochloride 5
mg / mL rinse 3-4 times.
Fluid replacement
Acyclovir 5% cream local application
3-4 times for 7 days
41.
41
• Severe cases• Acyclovir 200 mg – 400
mg 5 times a day for 7
days
• Valacyclovir 1g twice for
7 days
• Famciclovir 500mg
thrice for 7 days.
42.
42
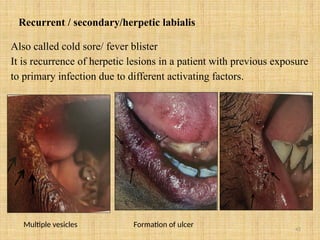
Recurrent / secondary/herpeticlabialis
Also called cold sore/ fever blister
It is recurrence of herpetic lesions in a patient with previous exposure
to primary infection due to different activating factors.
Multiple vesicles Formation of ulcer
43.
43
pathogenesis
The viruses, oncethey have been introduced into the body ( primary herpetic infection)
Appear to reside dormantly / latent within the regional ganglia
When appropriate trigger occurs ( sunlight, trauma, stress) virus reactivates ,replicates
in the ganglion And travels along ganglion to the skin / mucosal site
The virus travels down the axon to the periphery and infects the epithelial cells adjacent
to the cutaneous nerve endings.
The virus causes the epithelial cells to enlarge to form multi- nucleated giant cells
( Tzank cells)
Causes cells lysis and formation of vesicles.
44.
44
Clinical features
• Age/gender– adult
• Female > male
• Site – at the site of primary inoculation
• Adjacent area supplied by involved ganglion
• On lips
• Intraorally – mucosa tightly bound to periosteum
• ( hard palate, attached gingiva , alveolar ridge)
46
Investigation
• Detection ofviral DNA
• Antibody titres/
serological methods
• Most sensitive &
accurate method is PCR
technique.
• Detection of antibody
against herpes.
47.
47
Investigations
• Cytosmear/exfoliative
cytology
• Isolation& tissue culture
• Scrappings of lesion , stain
with Wright`s, giemsa stain,
PAP stain
• Demonstrates balloon cells,
multinucleated giant cells &
intranuclear inclusions bodies.
• Isolation of virus in tissue
culture, by DNA scappings
from lesions.
48.
48
Treatment
To relieve pain
Tomaintain
proper fluid
Balance
Mild – moderate
cases
Analgesics topical / systemic
Diphenhydramine hydrochloride 5
mg / mL rinse 3-4 times.
Fluid replacement
Acyclovir 5% cream local
application 3-4 times for 7 days
49.
49
• Severe cases• Acyclovir 200 mg – 400
mg 5 times a day for 7
days
• Valacyclovir 1g twice for
7 days
• Famciclovir 500mg
thrice for 7 days.
50.
50
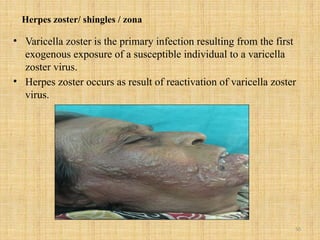
Herpes zoster/ shingles/ zona
• Varicella zoster is the primary infection resulting from the first
exogenous exposure of a susceptible individual to a varicella
zoster virus.
• Herpes zoster occurs as result of reactivation of varicella zoster
virus.
51.
51
pathogenesis Chicken poxis the varicella zoster infection in a person who is
Not exposed earlier
Following infection , varicella zoster enters sensory nerve endings ans is then transported
By retrograde axonal transport to the neuronal cell bodies along nerve pathway
The virus reaches nerve ganglia and remains latent there until reactivated
When an appropriate trigger occurs virus reactivates, replicates in the ganglion
Travels along axons to skin/ mucosa causing cluster of smaller erythematous papule
With rashes , burning sensation and tingling
The rashes develops into small vesicle pus crust formation and healing (4-5 weeks)
Sometimes pain continues for more than 3-4 months called post herpetic neuralgia
52.
52
Clinical course -
Pain– boring , pricking, itching , burning, rashes headache, malaise
Are present 1-4 days
Inflammatory reaction will result in the development of cluster of vesicles on
erythematous base (acute phase)
Within 3-4 days , vesicles become pustular and ulcerate and crusts after 7-10 days
The lesions tend to follow the path of affected nerve and terminate at the midline.
After acute phase resolution of the lesion occurs in 2- 3 weeks with scarring ,
hypo pigmentation or hyper pigmentation.
About 15% cases may proceed to chronic phase with neuralgia associated pain
Persists longer than 3 months called post herpitic neuralgia.
53.
53
If it affects
Maxillarydivision
The lesions are localized to
areas including cheek, lower
eyelid, side of nose, upper
lid, upper teeth are, mucous
membrane of nose,
nasopharynx, tonsils, roof of
the mouth.
Mandibular division
It involves the sides of the
head, part of the external
ear, auditory canal, the
lower lip and part of the
mucosa of the mouth.
54.
54
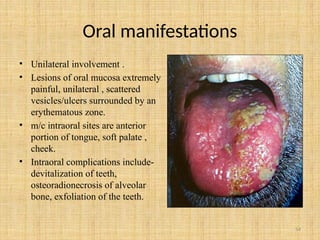
Oral manifestations
• Unilateralinvolvement .
• Lesions of oral mucosa extremely
painful, unilateral , scattered
vesicles/ulcers surrounded by an
erythematous zone.
• m/c intraoral sites are anterior
portion of tongue, soft palate ,
cheek.
• Intraoral complications include-
devitalization of teeth,
osteoradionecrosis of alveolar
bone, exfoliation of the teeth.
56
Investigations
• Complete hemogram
•Cytology – tzank smear test
• Biopsy
• Virological tests – viral culture
isolation & neutralization of virus
Serologic tests: complement fixation test
immunofluorescent test
VZV membrane antigens
Molecular methods : PCR
Elisa
57.
57
Treatment
• To relievepain • Topical analgesics –
• Lignocaine patch : 5% patch
• EMLA cream ( eutectic mixture of
lidocaine 2.5% & prilocaine 2.5%
• Capsaicin cream – 0.025 – 0.075%
• Systemic analgesics –
• Paracetamol/acetaminophen 500 mg
3-4 times a day
• Ibuprofen 400 mg 3-4 times a day
58.
58
• To decreaseviral load
• To relieve chronic pain and
to prevent chances of post
herpetic neuralgia
Antiviral therapy –
Acyclovir – 800 mg , orally 5
times a day for 7-10 days
Valacyclovir – 1000 mg tid for
7 days
Famciclovir – 500 mg three
times daily
Tricyclic antidepressants-
Amitriptyline 10 – 25 mg
orally at bedtime , increase
dosage by 25 mg every 2-4
weeks.
59.
59
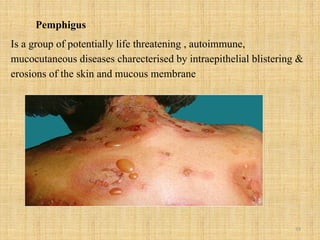
Pemphigus
Is a groupof potentially life threatening , autoimmune,
mucocutaneous diseases charecterised by intraepithelial blistering &
erosions of the skin and mucous membrane
60.
60
Pathogenesis -
Presence ofautoantibodies (IgG,IgA)
React with desmosomal glycoproteins ( desmoplakin, desmogleins)
Which are present on the cell surface of the keratinocyte
( desmosomes causes cell to cell adhesion in the epithelium.
The immune system reaction against these glycoproteins causes a loss of cell to cell
Adhesion
Resulting in the formation of intraepithelial bullae due to acatholysis ( breaking of
Stratum spinosum)
Since oral epithelium epresses largely Dsg 3 , but skin expresses Dsg 1 as well as Dsg3
Damage to Dsg 3 results in oral lesions at an early stage , while damage to Dsg 1 results
In skin lesions 1
63
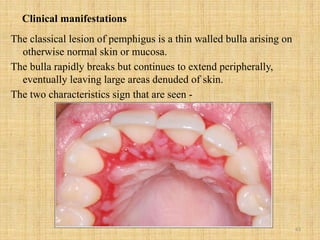
Clinical manifestations
The classicallesion of pemphigus is a thin walled bulla arising on
otherwise normal skin or mucosa.
The bulla rapidly breaks but continues to extend peripherally,
eventually leaving large areas denuded of skin.
The two characteristics sign that are seen -
64.
64
sign
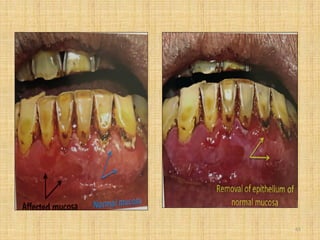
Nikolsky sign
mechanism
The applicationof pressure to
apparently normal skin in the
surrounding area of a vesicle
resulting in the removal of upper
layer of epidermis and fromation
of new lesion.
Two types o nikolsky sign are
described-
1) Wet – base of the skin is moist ,
glistening & exudative
suggestive of active disease
2) Dry – base of eroded skin is
relatively dry suggestive of
active disease healing lesion.
66
• Asboe hansensign/
bulla spreading sign
• Marginal nikolsky sign
• On application of pressure to an
intact bulla, the bulla enlarges by
extension to an apparently normal
surface
• Application of lateral pressure to
a pre- existing lesion using a
cotton tipped swab , tongue
depressor leads to lateral
extension of bulla.
67.
67
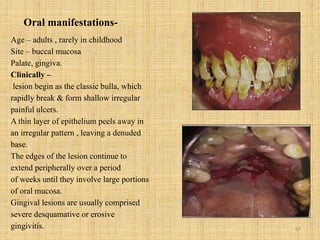
Oral manifestations-
Age –adults , rarely in childhood
Site – buccal mucosa
Palate, gingiva.
Clinically –
lesion begin as the classic bulla, which
rapidly break & form shallow irregular
painful ulcers.
A thin layer of epithelium peels away in
an irregular pattern , leaving a denuded
base.
The edges of the lesion continue to
extend peripherally over a period
of weeks until they involve large portions
of oral mucosa.
Gingival lesions are usually comprised
severe desquamative or erosive
gingivitis.
68.
68
Differential diagnosis
1) Mucousmembrane pemphigoid –
Pemphigus shows positive Nikolsky and Asboe Hensen sign while
absent in pemphigoid
It manifest in other mucous like eye, genital etc.
2) Erythema multiforme - pemphigus shows positive nikolsky and
asboe hensen sign absent in EM
EM target lesion , absent in pemphigus
Pemphigus extends central to peripheral . While EM from peripheral
to central.
69.
69
Investigations
Biopsy of perilesionaltissue & histological & immunostaining
Examination
Assay of serum antibody titres by direct and indirect
Immunofluorescence
ELISAs for detection of antibodies to desmoglein 1 & 2
70.
70
Treatment
condition
• Very milddisease
(Oral lesions)
• Moderate cases
( oral pemphigoid +
skin lesions)
Drug with doses
Topical corticosteroids –
Fluocinonide – 0.05% 2-3 applications
Daily.
Clobetasol proprionate 0.05% (2-3
applications per day).
Prednisolone doses of 40-60 mg daily.
71.
71
More severe cases
Ifprednisolone doses
Above 100 mg daily are
Unresponsive (pulsed intra
venous therapy)
• Prednisolone doses 60- 100
mg ( 1- 2 mg/kg/day)
• Pulsed intravenous therapy
with 1 g of methyl
prednisolone in 150 mL of
dextrose and water,
administered over a period
of 90 min once daily , on 1-
5 consecutive days, may be
considered.
72.
72
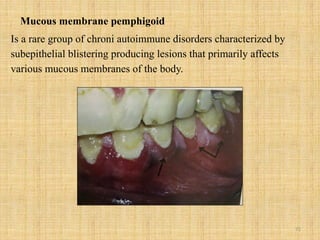
Mucous membrane pemphigoid
Isa rare group of chroni autoimmune disorders characterized by
subepithelial blistering producing lesions that primarily affects
various mucous membranes of the body.
73.
73
pathogenesis
Presence of autoantibodies(IgG,IgA,IgM)
Bind with hemidesmosomes or basement membrane gllycoproteins,
which will act as self antigen .
The immune reaction against these glycoproteins causes detachment of
the basal cells from the basement membrane zones
Resulting in the formation of subepithelial bullae
74.
74
Oral lesions
The orallesions may begin as classic bulla which rapidly break &
form shallow irregular painful ulcers.
• Nikolsky & Asboe Hensen sign – mostly negative
• Ocular lesions –
• Chronic conjuctivitis with symptoms of burning, irritation ,
photophobia and excess tearing.
• Vesicles & ulcerations is seen only in advances stage.
• Scarring following repeated fibrosis can lead to the fusion of the
bulbar and palpebral conjuctivae(symblepharon) or the superior &
inferior palpebrae (Ankyoblepharon)
75.
75
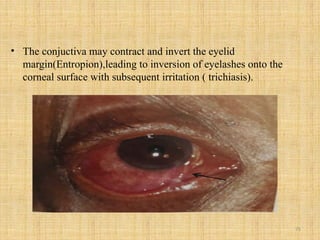
• The conjuctivamay contract and invert the eyelid
margin(Entropion),leading to inversion of eyelashes onto the
corneal surface with subsequent irritation ( trichiasis).
77
Treatment
condition
• Very milddisease
(Oral lesions)
• Moderate cases
( oral pemphigoid +
skin lesions)
Drug with doses
Topical corticosteroids –
Fluocinonide – 0.05% 2-3 applications
Daily.
Clobetasol proprionate 0.05% (2-3
applications per day).
Prednisolone doses of 40-60 mg daily.
78.
78
More severe cases
Ifprednisolone doses
Above 100 mg daily are
Unresponsive (pulsed intra
venous therapy)
• Prednisolone doses 60- 100
mg ( 1- 2 mg/kg/day)
• Pulsed intravenous therapy
with 1 g of methyl
prednisolone in 150 mL of
dextrose and water,
administered over a period
of 90 min once daily , on 1-
5 consecutive days, may be
considered.
79.
79
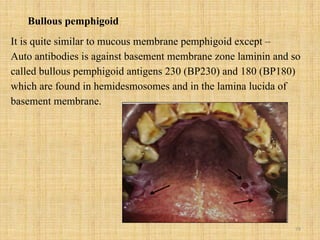
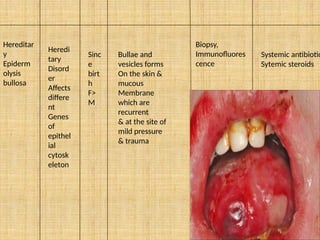
Bullous pemphigoid
It isquite similar to mucous membrane pemphigoid except –
Auto antibodies is against basement membrane zone laminin and so
called bullous pemphigoid antigens 230 (BP230) and 180 (BP180)
which are found in hemidesmosomes and in the lamina lucida of
basement membrane.
80.
80
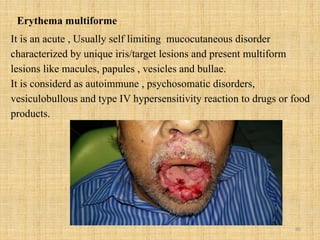
Erythema multiforme
It isan acute , Usually self limiting mucocutaneous disorder
characterized by unique iris/target lesions and present multiform
lesions like macules, papules , vesicles and bullae.
It is considerd as autoimmune , psychosomatic disorders,
vesiculobullous and type IV hypersensitivity reaction to drugs or food
products.
82
Pathogenesis
Presence of cellantigen ( viral DNA fragment , drug , metabolites etc.
Stimulation of CD4 T cells
Production of pro inflammatory mediators like interferon gamma and tumour necrosis
Factor alpha
Interferon gamma and TNF stimulates the production of additional cytokines and
Chemokines Cytotoxic T cells and natural killer cells
These cytotoxic T cells , NK cells or chemokines can all induce epithelial damage
So erythema multiforme appears to be the result of a cell – mediated immune
reaction to the precipitating agent
83.
83
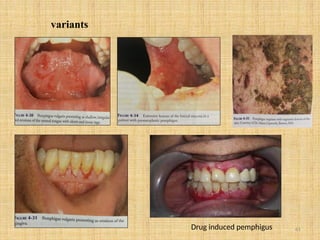
Variants
Erythema multiforme minor
Erythemamultiforme major
- Stevens johnson syndrome
- Toxic epidermal necrolysis
- Oral manifestations –
- Oral manifestation of EM minor is less than EM major
- Oral lesions may be found on lips , labial mucosa, floor of mouth ,
soft palate , buccal , gingival mucosa
- Clinical stages – the development of oral lesions can be divided
into 5 stages :- Macular , vesicular , sloughing ,pseudomembranous
And healing
84.
84
Lips are extensivelyinvolved with crust formation
Dysphagia if lesions are present on oropharynx
Presence of enlarged lymph nodes.
1) Steven johnson syndrome –
More severe than EM minor and major
Involves multiple mucous membranes – oral cavity , the genital ,
ocular , laryngeal and oesophageal mucosa.
Skin – epidermal attachment > 10 % with atypical flat target lesion
Systemic involvement is also seen.
Mucosal vesicles and bullae occur which ruptures and leave surface
Covered with thick white or yellow exudates.
Lips may exhibit bloody crusting which are extremely painful.
86
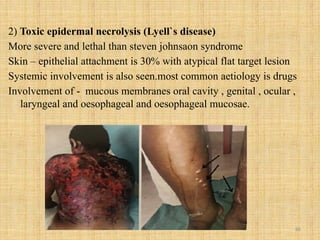
2) Toxic epidermalnecrolysis (Lyell`s disease)
More severe and lethal than steven johnsaon syndrome
Skin – epithelial attachment is 30% with atypical flat target lesion
Systemic involvement is also seen.most common aetiology is drugs
Involvement of - mucous membranes oral cavity , genital , ocular ,
laryngeal and oesophageal and oesophageal mucosae.
87.
87
.
Typical targets
Raised
atypical
targets
Is definedas individual lesion
less then 3 cm in diameter
Regular round shaped, well
defined border , two concentric
palpable
Oedematous rings , paler than
the centre.
Similar to target lesions and is
palpable erythematous lesions
with a rounded shape but poorly
defined borders and a dark
central area which may erode
and become necrotic.
These lesions are more
common in EM minor.
Common in EM major
And SJS.
Different target lesion in different variety
88.
88
Flat atypical targets
Flatatypical
targets – as
their name
suggests are not
palpable
And they form
ill- defined
erythematous
areas with a
tendency
To central
blister
formation.
These lesions are most
common
In SJS.
90
Invetigations for allforms of EM
Erythema multiforme is diagnosed clinically.
In patients who have target lesions with a preceding or coexisting HSV
infection , the diagnosis can be made easily.
immunofluorescence can be useful in some cases.
Differential diagnosis for oral lesions for all forms of EM
Primary herpetic stomatitis
Pemphigus
Mucous membrane pemphigoid
91.
91
Treatment
• Mild formsMild cases heal in 2-6 weeks
Local wound care
Topical analgesics
Diphenhydramine hydrochloride syrup
mixed with equal amount of antacid
liquid in a swish and swallow method
3-4 times daily.
Topical steroids – clobetasol
Proprionate 0.05%, triamcinolone
acetonide – 0.1% - apply 3-4 times a
Day.
92.
92
For more severecases
(for EM major & SJS)
If patient is resistant
unresponsive or
allergic to steroid
In cases suspecting
herpes suspecting
herpes associated EM
Systemic corticosteroids
Prednisolone 60 – 100 mg
daily ( 1- 2 mg / kg /day)
Immunosuppressive drugs /
steroid sparing drugs .
Azathioprine,
cyclophosphamide ,
cyclosporine , methotrexate
Acyclovir ( 400 mg twice / day)
Valacyclovir (500-1000mg/day)
Famciclovir (125-250mg/day)
93.
93
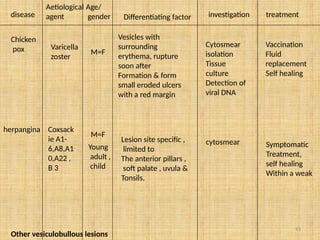
disease
Aetiological
agent
Age/
gender Differentiating factorinvestigation treatment
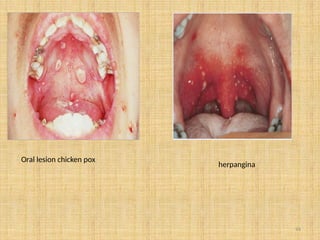
Chicken
pox Varicella
zoster
M=F
Vesicles with
surrounding
erythema, rupture
soon after
Formation & form
small eroded ulcers
with a red margin
Cytosmear
isolation
Tissue
culture
Detection of
viral DNA
Vaccination
Fluid
replacement
Self healing
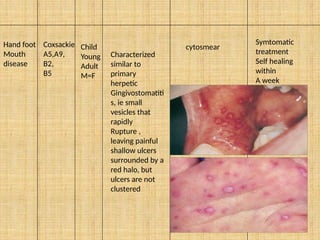
herpangina Coxsack
ie A1-
6,A8,A1
0,A22 ,
B 3
M=F
Young
adult ,
child
Lesion site specific ,
limited to
The anterior pillars ,
soft palate , uvula &
Tonsils.
cytosmear Symptomatic
Treatment,
self healing
Within a weak
Other vesiculobullous lesions
97
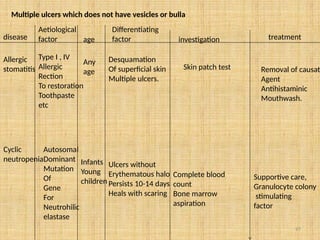
Multiple ulcers whichdoes not have vesicles or bulla
disease
Aetiological
factor age
Differentiating
factor investigation treatment
Allergic
stomatitis
Type I , IV
Allergic
Rection
To restoration
Toothpaste
etc
Any
age
Desquamation
Of superficial skin
Multiple ulcers.
Skin patch test Removal of causati
Agent
Antihistaminic
Mouthwash.
Cyclic
neutropenia
Autosomal
Dominant
Mutation
Of
Gene
For
Neutrohilic
elastase
Infants
Young
children
Ulcers without
Erythematous halo
Persists 10-14 days
Heals with scaring
Complete blood
count
Bone marrow
aspiration
Supportive care,
Granulocyte colony
stimulating
factor
99
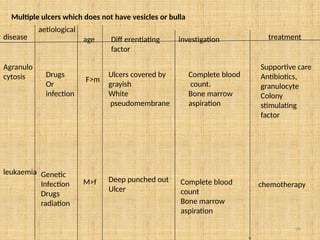
Multiple ulcers whichdoes not have vesicles or bulla
disease
aetiological
age Diff erentiating
factor
investigation treatment
Agranulo
cytosis Drugs
Or
infection
F>m
Ulcers covered by
grayish
White
pseudomembrane
Complete blood
count.
Bone marrow
aspiration
Supportive care
Antibiotics,
granulocyte
Colony
stimulating
factor
leukaemia Genetic
Infection
Drugs
radiation
M>f Deep punched out
Ulcer
Complete blood
count
Bone marrow
aspiration
chemotherapy