- The human body is inhabited by many microorganisms, mostly bacteria, that normally do not cause harm and may provide benefits. These make up the normal microbiota.
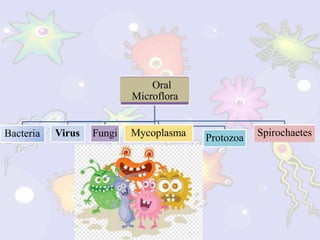
- The oral cavity specifically contains a variety of microbes including bacteria, viruses, fungi and protozoa. In infancy, colonization begins with bacteria like streptococcus salivarius transmitted from caregivers.
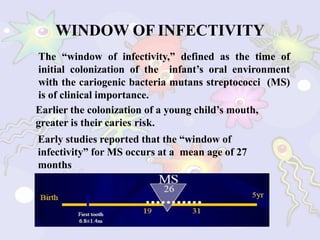
- As teeth erupt, the microbiota becomes more complex with bacteria like streptococcus mutans and increases in anaerobic bacteria. The "window of infectivity" for mutans streptococci transmission is between 19-31 months of age, making early childhood an important time for preventing cavities.