Downloaded 479 times

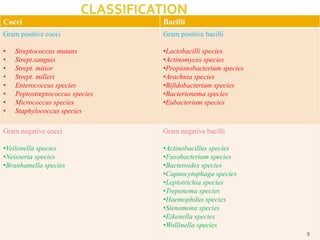
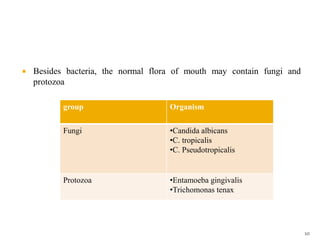
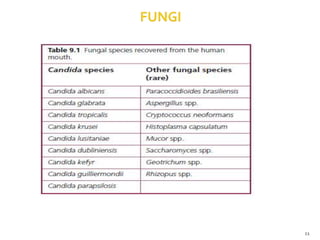
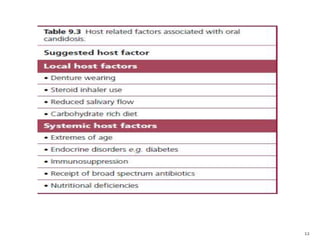
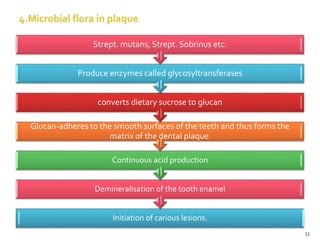
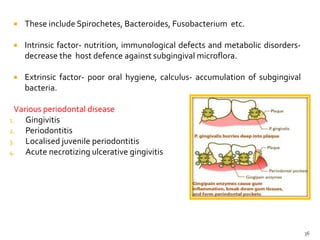


The document discusses the oral microbiota and its role in various oral diseases. It begins with an introduction to oral microbiology and a brief history. It then describes the normal microbial flora of the oral cavity including bacteria, fungi and protozoa. Several key bacteria associated with dental diseases like dental caries and periodontal disease are mentioned. The document also discusses the development of oral flora from infancy to adulthood. Various diseases caused by oral microbes like dental plaque, caries, periodontitis and endodontic infections are summarized. Sample collection and diagnostic methods for oral pathogens are also outlined.












































































