Huang et al.in 1999.
Imaging technique that uses low-coherence (near-infrared light)
long wavelength light penetrate into the scattering medium.
Cross-sectional imaging of the microscopic structure of biological tissues
Superluminescent diode or Femtosecond lasers (which have very short
pulses)
3D imaging reconstruction through intrinsic contrasting of back-scattered
(coherent) light
Higher resolution (less than 10 μm axially and less than 20 μm laterally) than
other imaging modalities such as MRI or ultrasound.
Optical Coherence Tomography
3.
The key benefitsof OCT are:
Live sub-surface images at near-microscopic resolution
Instant, direct imaging of tissue morphology
No preparation of the sample or subject, no contact
No ionizing radiation
higher resolution (because it is based on light, rather than
sound or radio frequency)
low near-infrared safe for eye
Better penetration than light microscopes (despite lower
resolution
4.
Optical Coherence Tomography
Opticalcoherence tomography (OCT) is a non-invasive, non-contact imaging
system providing high resolution cross-sectional images of the posterior
segment. OCT is analogous to B-scan ultrasonography but uses near-infrared
light interferometry rather than sound waves, with images created by the
analysis of inter-ference between reflected reference waves and those reflected
by tissue. Most instruments in current use employ spectral/Fourier domain
technology, in which the mechanical movement required for image acquisition in
older ‘time domain’ machines have been eliminated and the information for each
point on the A-scan is collected simultaneously, speeding data collection and
improving resolution. Promising newer modalities include swept-source (SS) OCT
that can acquire images at a much higher rate and with extremely high retinal
element resolution and better imaging depth. So-called ‘adaptive optics’ allows
correction of higher-order optical aberrations to improve resolution. Wide-field,
intraoperative, functional and Doppler (blood flow measurement) OCT
applications may all have clinical utility in the future. The diagnosis and
monitoring of macular pathology has been revolutionized by the advent of OCT
imaging, e.g. AMD, diabetic maculopathy, macular hole, epiretinal membrane
and vitreo-macular traction, CSR and retinal venous occlusion. This technology
5.
Normal appearance
High reflectivitystructures can be depicted in a pseudo-colour image as red,
intermediate as green-yellow and low reflectivity as blue-black. Fine retinal structures
such as the external limiting membrane and ganglion cell layer can be defined . Detailed
quantitative information on retinal thickness can be displayed numerically and in false-
colour topographical maps. Three-dimensional images can be constructed, and different
retinal layers studied in relief
OCT imaging. (A) High resolution image provided by spectral-domain OCT; (B) spectral-domain image of the
macula (using false colour): CC = choriocapillaris; ELM = external limiting membrane; GCL = ganglion cell layer;
INL = inner nuclear layer; IPL = inner plexiform layer; IS/OS = photoreceptor inner-segment/outer-segment
junction (also called ellipsoid zone); MZ = myoid zone; NFL = nerve fibre layer; ONL = outer nuclear layer; OPL =
outer plexiform layer; PRO = photoreceptor outer segments; RPE = retinal pigment epithelium
6.
OCT-angiography
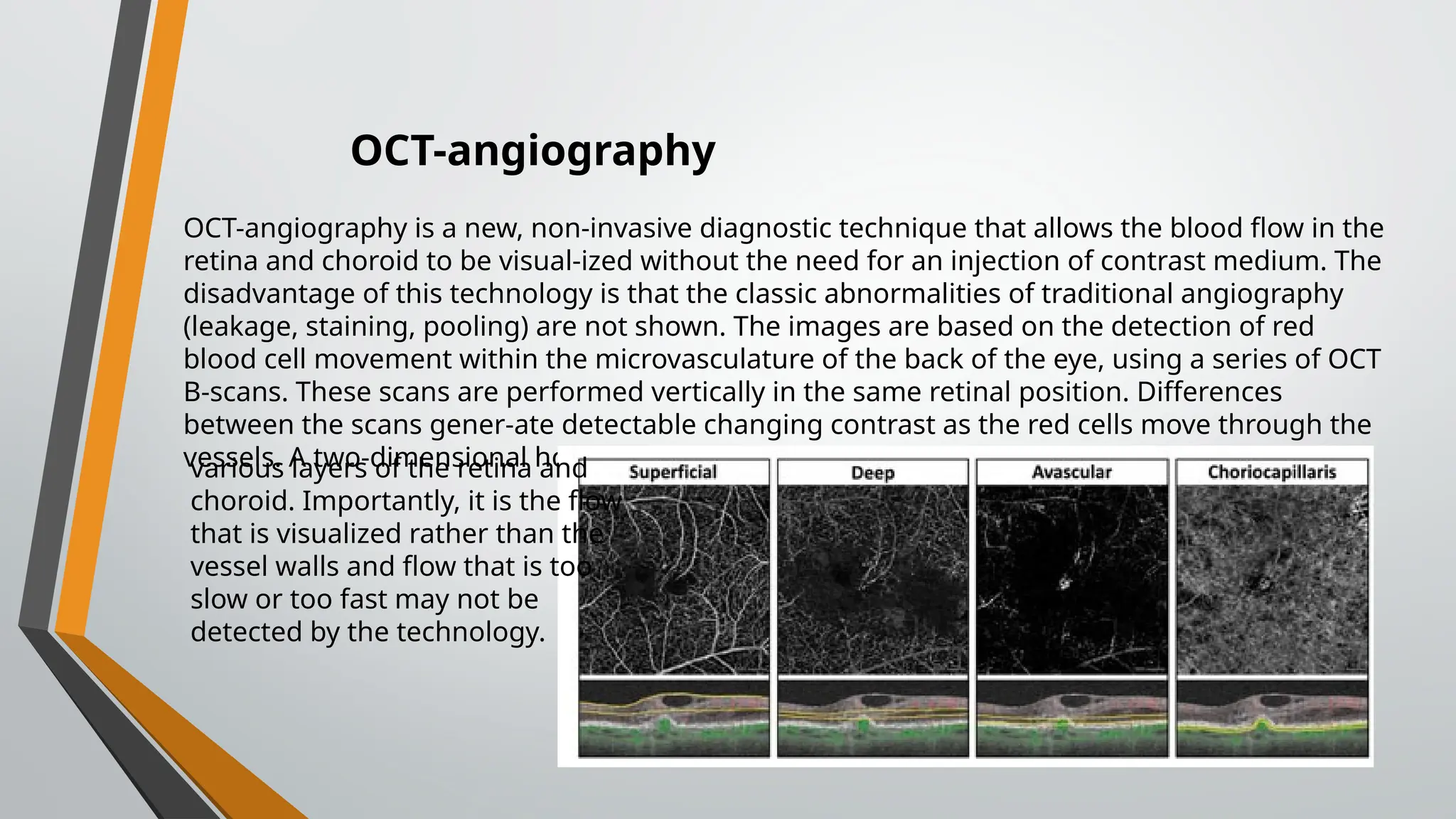
OCT-angiography is anew, non-invasive diagnostic technique that allows the blood flow in the
retina and choroid to be visual-ized without the need for an injection of contrast medium. The
disadvantage of this technology is that the classic abnormalities of traditional angiography
(leakage, staining, pooling) are not shown. The images are based on the detection of red
blood cell movement within the microvasculature of the back of the eye, using a series of OCT
B-scans. These scans are performed vertically in the same retinal position. Differences
between the scans gener-ate detectable changing contrast as the red cells move through the
vessels. A two-dimensional horizontal map is then created of the microcirculation, within the
various layers of the retina and
choroid. Importantly, it is the flow
that is visualized rather than the
vessel walls and flow that is too
slow or too fast may not be
detected by the technology.
7.
Applications
• Diagnosis ofa choroidal neovascular membrane:
○ Visualization of flow in the outer retina.
○ Abnormal vasculature in areas featuring blood
vessels
• In dry AMD to diagnose a non-exudative choroidal
neovascu-lar membrane.
• Visualization of abnormal choroidal vessels,
particularly after treatment.
• Diabetic retinopathy:
○ Diagnosis of preretinal neovascularization and to
differ-entiate intraretinal microvascular
abnormalities (IRMA) from new vessels.
○ Detection of microvascular changes without clinical
retinopathy.
○ To assess the deep retinal capillary plexus in
macular oedema.
○ To assess the microcirculation in patients with
macular ischaemia
OCT-angiography. (A) FA showing choroidal
neovascular membrane; (B) OCT angio-gram of
(A); (C) FA at 2 minutes in diabetic macular
oedema; (D) OCT angiogram of deep capillary
plexus showing loss of the perifoveal network;
(E) FA late phase showing polypoidal choroidal
vasculopathy; (F) OCT angiogram; the black
area is a polyp (arrow) and does not show
vascularization because of turbulence within
the polyp (Courtesy of A Ambresin)
8.
Color Fundus ImagingOCT and. The 2D Image of the Retina
Fundus photography can be used only for visualizing the 2-dimensional view of the retina and lacks
providing depth information about the retinal layer .The interferometric technique’s properties are
defined by the signal sampling at the detector and the light source’s coherence properties. With this
unique OCT property, the retina’s high-resolution image is achieved
Timed domain OCT and Frequency domain OCT are different type of acquisition domains. The
light source used in TD-OCT is usually a super luminescent diode and reference beam length is
varied. Frequency domain OCT (FD-OCT) uses separate detectors to acquire the broadband
interference.
Timed Domain OCT and Frequency Domain OCT
9.
A photodiode producesa single frequency infrared
wave that is in phase with the optical processes. Next,
the transmitted beam is divided into two parts by
passing through the light diffuser. The first part, which
goes towards the tissue, is sent by the mirror to the
desired coordinates on the page and is focused at the
desired point by the lens. The second part is the
reference beam that determines the imaging depth by
a moving mirror. On the return path, both beams are
gathered together and go to the detector, where the
image is created based on the phase difference
between the return beam from the tissue and the
reference beam, as well as the autocorrelation function.
Time Domain OCT
10.
In the oppositefigures, you can see the two traveling
and reflected light waves.
Now consider two reflected light waves that meet and
converge at the detector. The optical power reached to
the detector by these two waves can be calculated
according to the following equation:
Light scattering ratio in interferometer
Mixed degree of convergence
The wave transmitted to the detector is strongly dependent on the time delay (phase
difference) of the two waves that have reached the detector. So that it can transfer more
power to the detector up to twice. The main idea of
the OCT imaging method also comes
from here.
Frequency Domain OCT
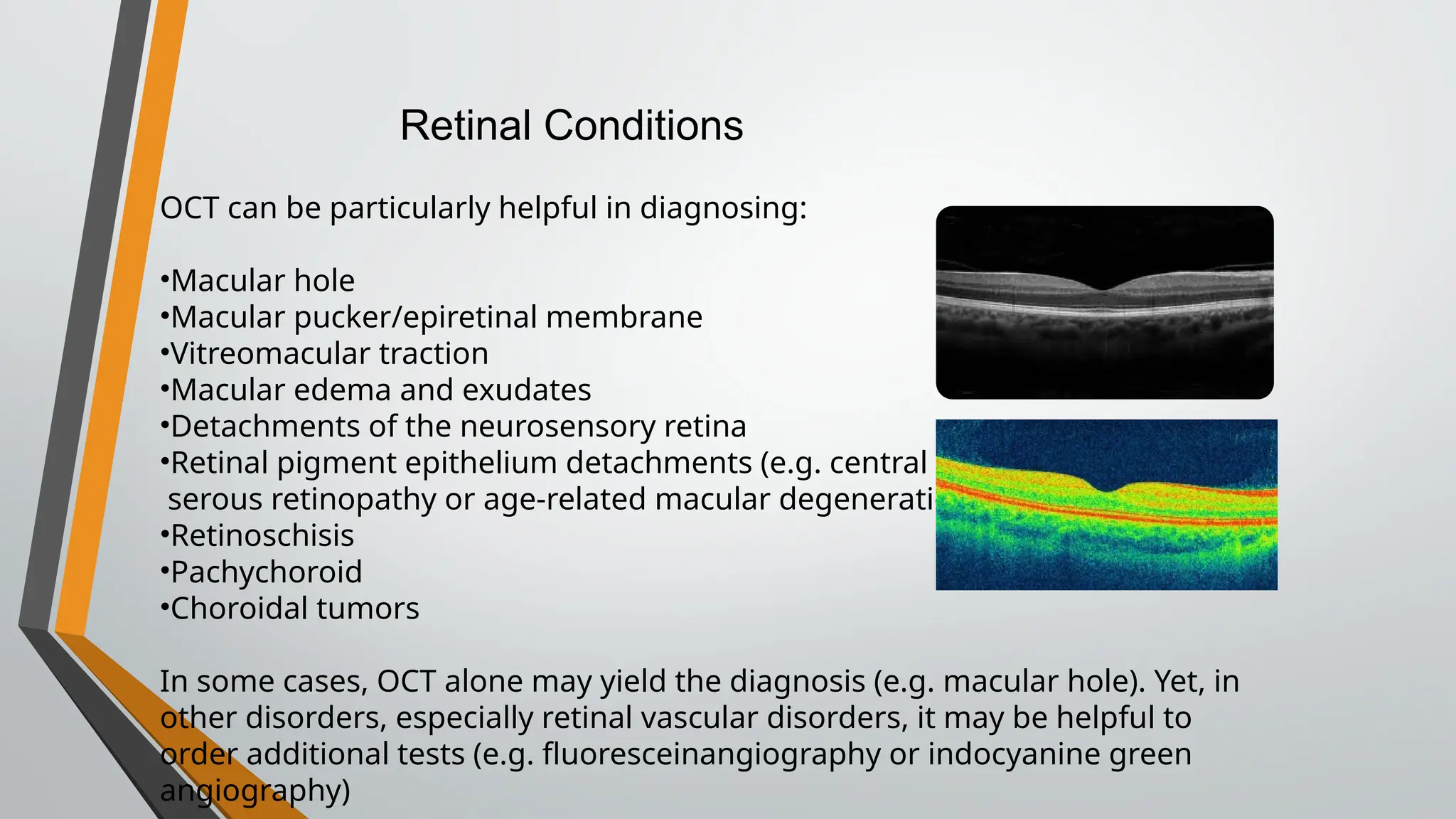
OCT can beparticularly helpful in diagnosing:
•Macular hole
•Macular pucker/epiretinal membrane
•Vitreomacular traction
•Macular edema and exudates
•Detachments of the neurosensory retina
•Retinal pigment epithelium detachments (e.g. central
serous retinopathy or age-related macular degeneration)
•Retinoschisis
•Pachychoroid
•Choroidal tumors
In some cases, OCT alone may yield the diagnosis (e.g. macular hole). Yet, in
other disorders, especially retinal vascular disorders, it may be helpful to
order additional tests (e.g. fluoresceinangiography or indocyanine green
angiography)
Retinal Conditions
Full thickness macularhole (a) OCT cross sectional image;
(b) color fundus photograph).
On OCT,
Stage 1 hole appears as a cystic
lesion in the inner layers of the
retina.
Stage 2 macular holes present as
a full-thickness defect at the
fovea (size < 400um in diameter).
Stage 3 macular hole is a
completely evolved hole (size
>400 um in diameter). In some
patients, a small operculum can
be seen suspended in front of the
lesion.
Stage 4 macular holes appear
similar to stage 3 holes except
that in stage 4 holes there
is complete posterior vitreous
detachment, as frequently
evidenced by a visible Weiss ring.
1. Macular Hole with OCT
The macula isthe portion of the retina responsible for
central vision. Occasionally, scar tissue grows on the surface
of the retina due to conditions that are not controllable or
preventable and causes wrinkling and swelling. This is known
as a macular pucker or epiretinal membrane (ERM). These
changes can lead to distortion of the central vision.
2.Macular Pucker/Epiretinal Membrane (ERM)
Vitreomacular traction (VMT) syndrome is a potentially
visually significant disorder of the vitreoretinal
interface characterized by an incomplete posterior
vitreous detachment with the persistently adherent
vitreous exerting tractional pull on the macula and
resulting in morphologic alterations and consequent
decline of visual function.
3. Vitreomacular traction (VMT)
17.
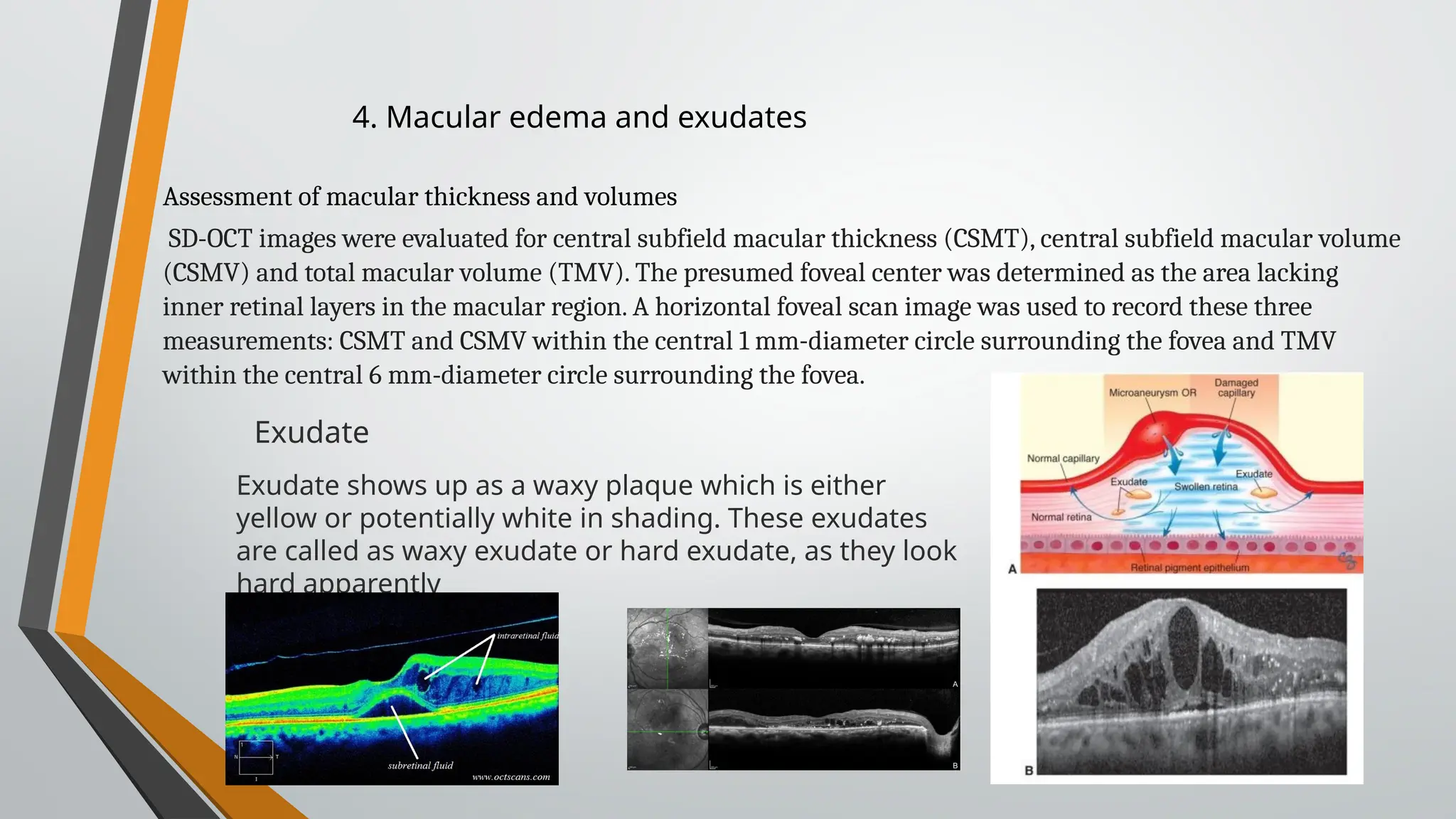
4. Macular edemaand exudates
SD-OCT images were evaluated for central subfield macular thickness (CSMT), central subfield macular volume
(CSMV) and total macular volume (TMV). The presumed foveal center was determined as the area lacking
inner retinal layers in the macular region. A horizontal foveal scan image was used to record these three
measurements: CSMT and CSMV within the central 1 mm-diameter circle surrounding the fovea and TMV
within the central 6 mm-diameter circle surrounding the fovea.
Assessment of macular thickness and volumes
Exudate shows up as a waxy plaque which is either
yellow or potentially white in shading. These exudates
are called as waxy exudate or hard exudate, as they look
hard apparently
Exudate
18.
5. Detachments ofThe Neurosensory Retina (RD)
Retinal detachment is a disorder of the eye in which
the retina peels away from its underlying layer of support
tissue. RD has 3 types;
• Rhegmatogenous retinal detachment –a hole or tear in
the retina that allows fluid to pass from the vitreous space
into the subretinal space between the sensory retina and
the RPE.
• Exudative, serous, or secondary retinal detachment –
inflammation, injury or vascular abnormalities that results in
fluid accumulating underneath the retina without the
presence of a hole, tear, or break.
• Tractional retinal detachment –fibrovascular tissue,
caused by an injury, inflammation or neovascularization, pulls
the sensory retina from the retinal pigment epithelium.
19.
6.Retinal Pigment EpitheliumDetachments
Retinal pigment epithelial detachments (PEDs) are structural
splitting within the inner aspect of Bruch’s membrane
separating the retinal pigment epithelium (RPE) from the
remaining Bruch’s membrane.
7.Retinoschisis
Retinoschisis is a condition in which an area of the retina (the
tissue lining the inside of the back of the eye that transmits
visual signals to the optic nerve and brain) has separated
into two layers. The part of the retina that is affected by
retinoschisis will have suboptimal vision. This can occur in
different layers of the retina, and for different reasons.
(Juvenile X-linked & Degenerative retinoschisis)
20.
An abnormal andpermanent increase in choroidal
thickness often showing dilated choroidal vessels and
other structural alterations of the normal choroidal
architecture. Central serous chorioretinopathy is just
one of several pachychoroid-related macular
disorders.
8.pachychoroid
9. Choroidal Tumors
21.
Optic nerve
OCT isgaining increasing popularity when evaluating optic nerve
disorders by accurately and reproducibly evaluate the retinal nerve fiber
layer and ganglion cell layer thickness:
•Glaucoma
•Optic neuritis
•Non-glaucomatous optic neuropathies
•Alzheimer's disease
22.
OCTA of ahealthy person, centered in the optic
disc.
OCTA of a glaucomatous patient (darker greys and
bluer color are appreciated compared to a healthy
OCTA-related definitions :
· Vessel density (VD): the percentage of area occupied by
vessels, pictured by lighter tones of grey
· Whole-image VD: the VD detected in the entire scan ·
Peripapillary VD: the VD within a 750-µm-wide annulus
extending from the optic disc boundary.
· Parafoveal VD: the VD between two circles centered in
the fovea with diameters of 1 mm and 3 mm
· Perifoveal VD: the VD within diameters of 3 mm and 5
mm.
OCTA in Glaucoma
23.
Optical coherence tomographyof the anterior
segment: evaluation of angle-closure glaucoma.
Optical coherence tomography of the posterior
pole:
○ Peripapillary RNFL: Because different OCT devices use
different scanning protocols, caution should be taken
when comparing RNFL thickness between machines.
By using the Bruch membrane opening (BMO)rather
than the optic disc margin, centration of the imagine
can be enhanced. When assessing structural changes
over time, it is often difficult to distinguish between
glaucomatous change and measurement variability or
age-related structural loss. Up to 4 μm inter-test
fluctuation has been reported. A new defect, widening
normal angle closed
angle
OCT in Glaucoma
24.
○ Optic nervehead. Radial cross-sectional scans
permit an objective and repeatable assessment
of disc morphology, with reasonable
discriminatory value.
○ Ganglion cell complex (GCC) analysis involves
measurement of the thickness of the RNFL, the
ganglion cell layer and the inner plexiform layer
at the macula in an attempt to detect early
stage glaucomatous damage. This is as effective
for diagnosing glaucoma and assessing
progression as analysis of the RNFL. OCT signal
quality is good, particularly in the elderly and
diseased eye. It should be considered
supplementary to RNFL assessment .
○ Progression analysis software has been
introduced on several machines and provides a
computed assessment of the extent of damage
over time. Trend-based analysis using a number
of scans, measures the shape of change and is
particularly useful when confirming that
(A) At presentation
(B) after 2 years showing progressive RNFL thinning
26.
Optic atrophy refersto the late stage changes that take place in the optic nerve resulting from
axonal degeneration in the pathway between the retina and the lateral geniculate body,
manifesting with disturbance in visual function and in the appearance of the optic nerve head.
Optic neuritis
Classification of optic neuritis
Retrobulbar neuritis, in which the optic disc appears normal, at least initially, because the
optic nerve head is not involved. It is the most common type in adults and is frequently
associated with multiple sclerosis (MS).
• Papillitis is characterized by hyperaemia and oedema of the optic disc, which may be
associated with peripapillary flame-shaped haemorrhages (Fig. 19.8). Cells may be seen in the
posterior vitreous. Papillitis is the most common type of optic neuritis in children, but can also
affect adults.
• Neuroretinitis is characterized by papillitis in association with inflammation of the RNFL
and a macular star figure (see below). It is the least common type and is only rarely a
manifestation of demyelination.
27.
Demonstrates sub-and intraretinalfluid
to a variable extent.
Patients show peripapillary retinal thinning.
Unaf-fected carriers frequently show variable
thickening of the temporal RNFL, perhaps
due to compensatory mitochondrial
accumulation.
Ay mshow peripapillary RNFL thickening and
will help to exclude macular pathology.
28.
OPTICAL COHERENCE TOMOGRAPHYAND ALZHEIMER DISEASE (A’D and OCT)
1.In terms of RNFL thickness, numerous studies have shown that most RNFL
parameters were reduced in patients with AD, especially those with cognitive
impairment.
Although there is some variation in which and how many quadrants are reduced, there
has been consistency in the results, even across different OCT machines, that show a
degree of RNFL thinning associated with AD patients when compared to healthy,
nondiseased controls.
2.In terms of total macular thickness, there are similar results as well, although fewer
studies have analyzed this specific finding. Retinal thickness in all macular quadrants
along with mean total macular volume
was lower in AD patients
than in control subjects.
OCT image of Normal (left) and AD (right)
29.
Fourteen studies assessingOCT-A in preclinical
Alzheimer's disease (AD), mild cognitive impairment,
or AD were included. Exploratory meta-analyses
revealed a significant increase in the foveal avascular
zone area and a significant decrease in superficial
parafoveal and whole vessel density in AD, although
there was significant heterogeneity between studies.
Although certain OCT-A metrics may have the potential
to serve as biomarkers for AD, the field requires
further standardization to allow conclusions to be
reached regarding their clinical utility.
OPTICAL COHERENCE TOMOGRAPHY ANGIOGRAPHY AND ALZHEIMER
DISEASE (A’D and OCT-A)
30.
Anterior segment
Anterior segmentOCT utilizes higher wavelength light than traditional posterior
segment OCT. This higher wavelength light results in greater absorption and less
penetration. In this fashion, images of the anterior segment (cornea, anterior
chamber, iris and angle) can be visualized.
31.
The commonly usedquantitative parameters are as
follows:
1.Angle opening distance (in mm): Perpendicular
distance between a point 500µm (AOD 500) or 750 µm
(AOD750) anterior to the scleral spur and the opposing
iris.
2.Angle recess area (in mm2
): The triangular area (ARA
500 or 750) bounded by the AOD 500 or 750, the
anterior iris surface and the inner corneo-scleral wall
3.Trabecular space area (in mm2
): Trapezoidal area
(TISA 500 or 750) bounded by the AOD 500 or 750, the
anterior iris surface, the inner corneo-scleral wall and
the perpendicular distance between the scleral spur
and the opposing iris.
Several other quantitative parameters such as iris
thickness , anterior chamber width and lens vault
have also been described.
32.
In clinical glaucomapractice, ASOCT is useful as an adjunct to gonioscopy as well as a
substitute when gonioscopy is not feasible due to corneal pathology or lack of patient co-
operation. In addition, it is extremely useful as a patient education tool, especially when
laser peripheral iridotomy is being recommended. When compared to gonioscopy, OCT
has the advantages of being non-contact and can be performed under dark conditions
allowing angle assessment during physiological mydriasis. Based on the iris profile and
position of the lens with respect to anterior segment structures, mechanisms of angle
closure such as pupillary block and anterior lens vault can be discerned (Figure 2). It is
important to note that structures behind the iris cannot be visualized with OCT, hence
diagnosis of posterior mechanisms of angle closure such as iridociliary lesions and plateau
iris must be confirmed with ultrasound biomicroscopy. ASOCT is also more useful than
UBM for serial monitoring of the angle since approximate alignment with ocular
landmarks (such as iridotomies, iris nevi, conjunctival blood vessels etc.) can be performed
with ASOCT by utilizing the video image during OCT scan acquisition. It is important to
keep in mind that not all scan types are corrected for errors due to refraction of the OCT
scanning beam and comparisons must only be made between similar scan types. OCT may
also be used to visualize trabeculectomy blebs and anterior segment implants such as
drainage devices and keratoprosthesis – however, the clinical value in these situations
appears to be limited.
Clinical use in glaucoma
34.
Limitations
Because OCT utilizeslight waves (unlike ultrasound which uses
sound waves) media opacities can interfere with optimal imaging.
As a result, the OCT will be limited the setting of vitreous
hemorrhage, dense cataract or corneal opacities.
As with most diagnostic tests, patient cooperation is a necessity.
Patient movement can diminish the quality of the image. With
newer machines, acquisition time is shorter which may result in
fewer motion related artifacts.
The quality of the image is also dependent on the operator of the
machine. Early models of OCT relied on the operator to accurately
place the image over the desired pathology. When serial images
were acquired over time (e.g. during treatment for AMD with anti-
VEGF therapy), later images could be taken that were off axis
compared to earlier images. Newer technologies, such as eye
tracking equipment, limit the likelihood of acquisition error.