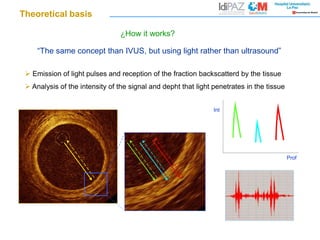
The document discusses optical coherence tomography (OCT) which uses light rather than ultrasound to image tissues. It provides the following key points:
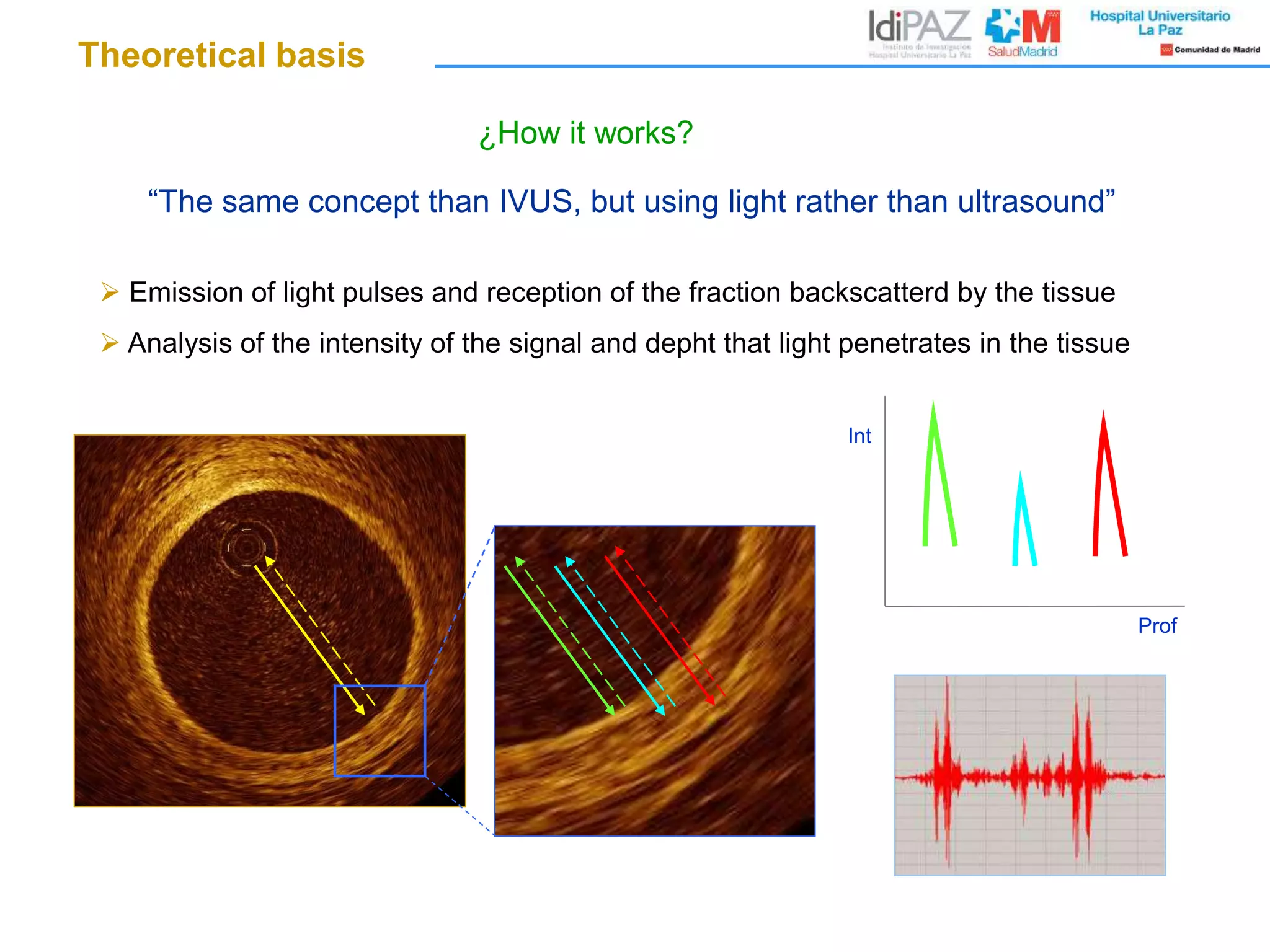
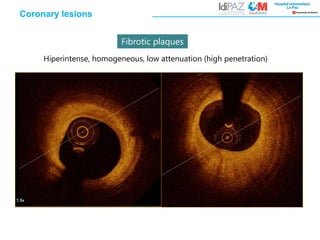
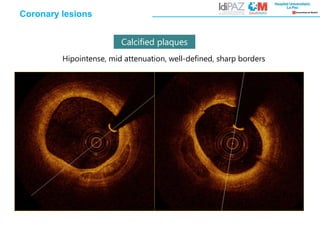
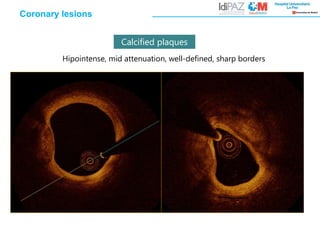
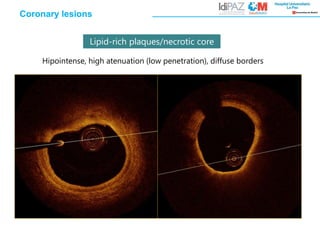
1. OCT emits light pulses into tissue and analyzes the intensity and depth of backscattered light to characterize tissues based on reflectivity and attenuation.
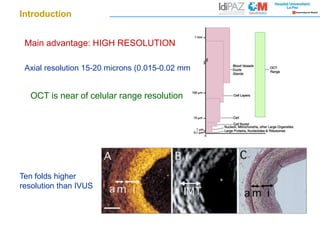
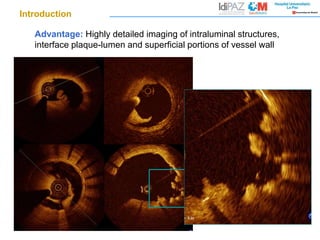
2. OCT provides higher resolution imaging of around 15-20 microns, around 10 times higher than intravascular ultrasound (IVUS), allowing detailed views of intraluminal structures.
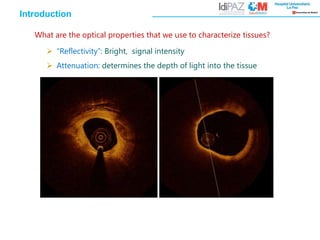
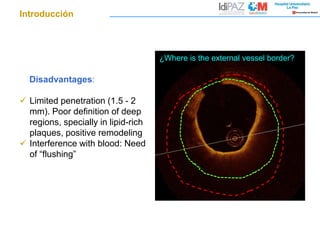
3. A limitation is its shallow penetration of around 1.5-2 mm, providing less definition of deep regions like lipid-rich plaques, requiring blood to be displaced for clear imaging.