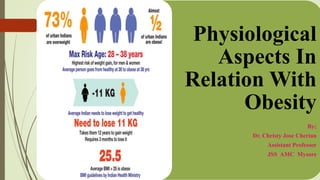
Physiological Aspects in Relation with Obesity discusses various topics related to obesity including:
- Meda dhatu, the physiological tissue responsible for fat storage and metabolism.
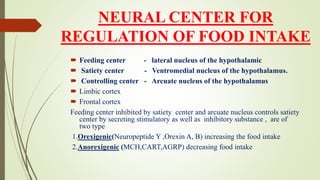
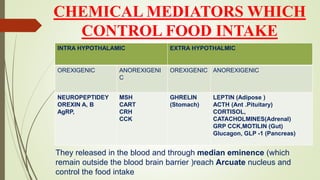
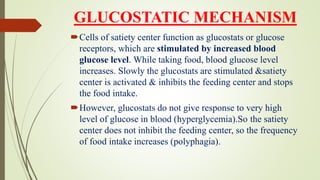
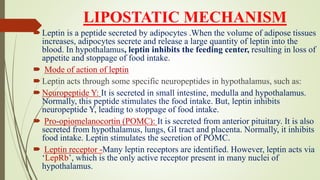
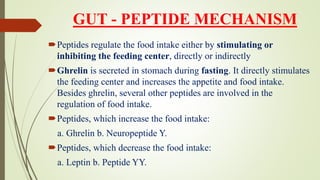
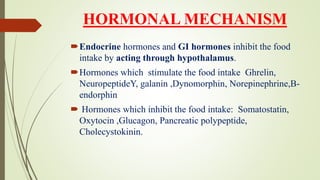
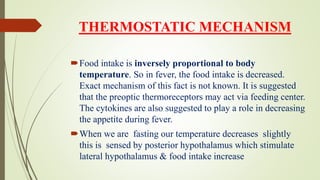
- Hunger and appetite regulation controlled by the hypothalamus and various hormones.
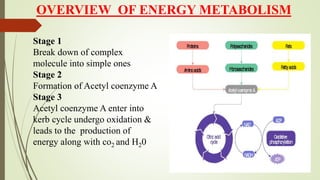
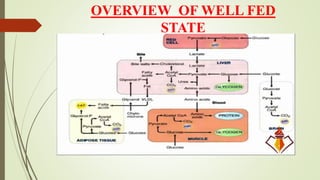
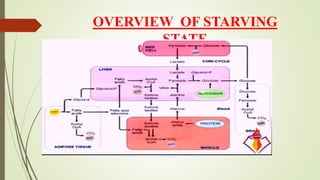
- An overview of energy metabolism including glycolysis, gluconeogenesis, and the citric acid cycle.
- Components of energy expenditure including basal metabolic rate, the thermic effect of food, and physical activity.