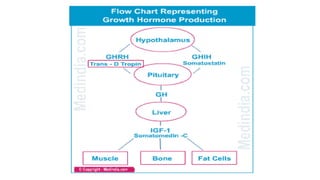
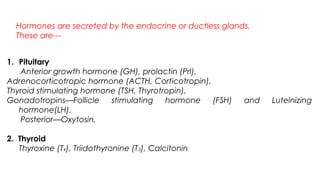
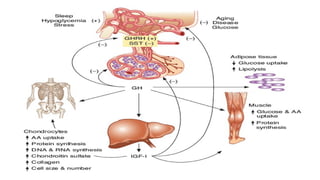
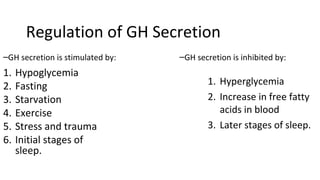
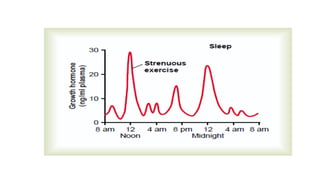
Growth hormone is synthesized by cells in the anterior pituitary gland and regulates growth, metabolism, and cell reproduction. It acts through somatomedins like insulin-like growth factor 1 to promote growth of bones and muscles. Growth hormone levels normally decrease with age but some people improperly use synthetic growth hormone in hopes of reversing aging or enhancing athletic performance, despite such uses not being approved by the FDA and having potential health risks. The presentation provided information on the synthesis, regulation, actions, and appropriate medical uses of growth hormone.