INTRODUCTION
Prenatal diagnosis isdefined as the method of detection of structural or
functional abnormalities in the developing foetus including genetic disorder
and congenital malformation detected by biochemical markers or by
ultrasound.
Most common - Down syndrome/ trisomy 21
2nd most common- Edward syndrome / trisomy 18
3rd most common - Patau syndrome/ trisomy 13
3.
(1) To enabletimely medical or surgical treatment of a condition before or after
birth
(2) To give the parents the chance to abort a fetus with the diagnosed condition
(3) To give parents the chance to prepare psychologically, socially, financially, and
medically for a baby with a health problem or disability, or for the likelihood of a
stillbirth.
(4) Prior information about problems in pregnancy means that healthcare staff as
well as parents can better prepare themselves for the delivery of a child with a
health problem.
PURPOSE OF PRENATAL EVALUATION
4.
CRITERIA FOR SCREENINGTESTS
• The test should be non-invasive and safe.
• It should be easily available.
• It should be simple and accurate.
• It should be inexpensive.
• It should be offered to all pregnant women.
• It should be performed for specific disorders with relatively high
prevalence with consideration of ethnic, racial and geographical
background
• Availability of prenatal diagnostic test should be there.
• There should be availability of treatment or management solution for
identified affected cases.
5.
INDICATION FOR PRENATALDIAGNOSIS
• I Prenatal risk factors-
• Age more than 35 years
• History of a congenitally malformed baby in the past.
• Previous child with chromosomal anomaly or unbalanced
translocation.
• Family history of congenital malformations like neural tube defects or
familial genetic diseases.
• Patient or partner being a carrier of chromosomal disorder, inversion
or translocation, etc.
• History of recurrent abortions in the past.
• Belonging to certain ethnic groups at high risk of certain congenital
diseases
6.
• II. Antenatalrisk factors in current pregnancy
• Exposure to certain infections like rubella, cytomegalovirus
• Intake of teratogenic drugs or exposure to teratogenic
environmental agents.
• Abnormal maternal serum biochemistry (Triple test)
• Uncontrolled maternal diabetes during periconceptional period or
raised glycosylated Hb.
• Presence of soft tissue markers for chromosomal anomalies or
structural defects on ultrasound.
• Amniotic fluid abnormalities like oligohydramnios or
polyhydramnios
• Severe symmetrical foetal growth restriction
• Decreased foetal activity
7.
TECHNIQUES FOR PRENATALDIAGNOSIS
1. History taking with pedigree chart
Detailed history about any congenital malformation or genetic disorder in the patient in the past or in the family is asked for.
Pedigree tree can be traced in presence of genetic disorders in the family.
2. First Trimester screening -
A. Maternal demography
B. 2. Ultrasonography
C. 3. Biochemical test
3. Second trimester screening
D. Biochemical test
E. Ultrasound
F. Integrated tests
4. Non invasive pre natal testing
3.Diagonstic Testing (Invasive Methods)
G. Chorionic villus sampling
H. Amniocentesis
I. Chordocentesis
J. Others
8.
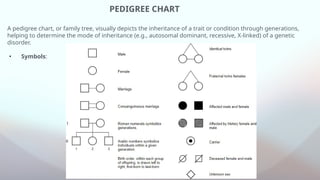
PEDIGREE CHART
A pedigreechart, or family tree, visually depicts the inheritance of a trait or condition through generations,
helping to determine the mode of inheritance (e.g., autosomal dominant, recessive, X-linked) of a genetic
disorder.
• Symbols:
9.
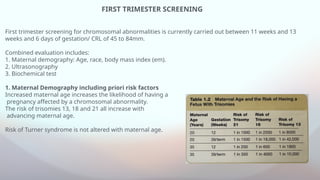
FIRST TRIMESTER SCREENING
Firsttrimester screening for chromosomal abnormalities is currently carried out between 11 weeks and 13
weeks and 6 days of gestation/ CRL of 45 to 84mm.
Combined evaluation includes:
1. Maternal demography: Age, race, body mass index (em).
2. Ultrasonography
3. Biochemical test
1. Maternal Demography including priori risk factors
Increased maternal age increases the likelihood of having a
pregnancy affected by a chromosomal abnormality.
The risk of trisomies 13, 18 and 21 all increase with
advancing maternal age.
Risk of Turner syndrome is not altered with maternal age.
10.
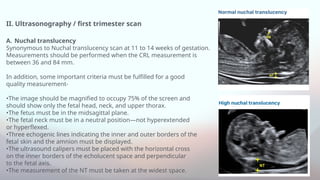
II. Ultrasonography /first trimester scan
A. Nuchal translucency
Synonymous to Nuchal translucency scan at 11 to 14 weeks of gestation.
Measurements should be performed when the CRL measurement is
between 36 and 84 mm.
In addition, some important criteria must be fulfilled for a good
quality measurement-
•The image should be magnified to occupy 75% of the screen and
should show only the fetal head, neck, and upper thorax.
•The fetus must be in the midsagittal plane.
•The fetal neck must be in a neutral position—not hyperextended
or hyperflexed.
•Three echogenic lines indicating the inner and outer borders of the
fetal skin and the amnion must be displayed.
•The ultrasound calipers must be placed with the horizontal cross
on the inner borders of the echolucent space and perpendicular
to the fetal axis.
•The measurement of the NT must be taken at the widest space.
11.
NT increases withgestational age even in the short-term window between the 10th and 14th weeks.
Therefore, NT values must be adjusted for gestational age.
Here, adjusting involves converting the NT to multiples of the median (MoM) for gestational age and using
either the 95th percentile for the MoM or the delta value of the observed NT from that expected for the
gestational age or crown-rump length.
However, it is also
important to note that an enlarged NT (greater than 3.0 mm) may be
considered an indication for diagnostic testing, regardless of gestational
age correction
12.
B. Nasal bone
Recentresearch has attempted to incorporate nasal bone evaluation
into current first trimester screening protocols in order to improve the
accuracy of aneuploidy diagnosis.
Including nasal bone measurement
improved the detection rate of Down syndrome to 90% and reduced
the false positive rate to 2.5%
C. Ductus venous Doppler study
Doppler study of the ductus venosus
normally will show triphasic, pulsatile forward flow. However, an
absent or reversed a wave during atrial systole has been observed in
cases of fetal cardiac malformations and aneuploidy.
In chromosomally normal fetuses with a normal NT, abnormal
ductus venosus blood flow in the first trimester has been associated
with adverse fetal outcome such as congenital heart disease and fetal
growth restriction.
D. Tricuspid regurgitation
The addition of tricuspid regurgitation to first tri-
mester serum screening and NT measurement has been shown to
increase the detection rate of Down syndrome from 91% to 96% at a
3% fixed false positive rate.
13.
Other anomalies tobe seen in first trimester
• Anencephaly
• Omphalocele.
• Gastroschisis.
• Posterior fossa defects.
• Spina bifida
• Facial cleft.
• Cardiac defects.
• Renal defects.
• Limb defects.
14.
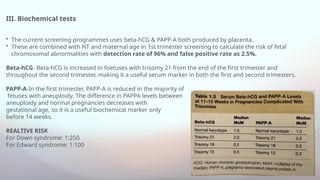
III. Biochemical tests
•The current screening programmes uses beta-hCG & PAPP-A both produced by placenta.
• These are combined with NT and maternal age in 1st trimester screening to calculate the risk of fetal
chromosomal abnormalities with detection rate of 96% and false positive rate as 2.5%.
Beta-hCG- Beta-hCG is increased in foetuses with trisomy 21 from the end of the first trimester and
throughout the second trimester, making it a useful serum marker in both the first and second trimesters.
PAPP-A-In the first trimester, PAPP-A is reduced in the majority of
fetuses with aneuploidy. The difference in PAPPA levels between
aneuploidy and normal pregnancies decreases with
gestational age, so it is a useful biochemical marker only
before 14 weeks.
REALTIVE RISK
For Down syndrome: 1:250
For Edward syndrome: 1:100
15.
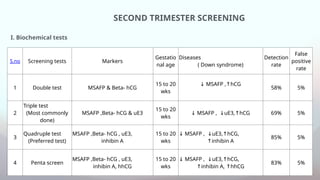
SECOND TRIMESTER SCREENING
S.noScreening tests Markers
Gestatio
nal age
Diseases
( Down syndrome)
Detection
rate
False
positive
rate
1 Double test MSAFP & Beta- hCG
15 to 20
wks
↓ MSAFP , hCG
↑
58% 5%
2
Triple test
(Most commonly
done)
MSAFP ,Beta- hCG & uE3
15 to 20
wks
↓ MSAFP , uE3, hCG
↓ ↑ 69% 5%
3
Quadruple test
(Preferred test)
MSAFP ,Beta- hCG , uE3,
inhibin A
15 to 20
wks
↓ MSAFP , uE3, hCG,
↓ ↑
↑inhibin A
85% 5%
4 Penta screen
MSAFP ,Beta- hCG , uE3,
inhibin A, hhCG
15 to 20
wks
↓ MSAFP , uE3, hCG,
↓ ↑
↑inhibin A, hhCG
↑
83% 5%
I. Biochemical tests
16.
II: ULTRASOUND
Look forsoft tissue markers: Positive if any 2 are present.
1. Nuchal sin fold thickness > or = 6 mm: Abnormal
2. Absent nasal bone,
3. Short humerus.
4. Short femur.
5. Simian crease.
6. Sandal gap.
7. Echogenic cardiac focus.
8. Echogenic bowel.
9. Pelvicalyceal dilatation.
10.Choroid plexus cyst.
If one positive :
◦ Highest risk : Nuchal skin fold thickness › Short femur.
◦ Lowest risk: Choroid plexus cyst.
17.
INTEGRATED TESTS
Combines resultsof first- and second-trimester tests
These serum markers, when combined with maternal age and nuchal translucency measurement is called as combined test.
It has 94 to 96% detection rate and 5% false positive rate for trisomy 21.
SEQUENTIAL SCREENING
It involves informing the patient of the results after first-trimester screening, with plan to offer prenatal diagnostic testing if the
calculated risk value lies above a specified threshold.
Stepwise sequential screening resulted in a 92-percent detection-rate and 5% false-positive rate for trisomy 21.
CONTINGENT SCREENING
Women are divided into high, moderate, and low-risk groups.
• Those at highest risk for trisomy 21 i.e. > 1:30 — are counselled and offered diagnostic testing.
• Women at moderate risk, between 1:30 and 1:1500, undergo second-trimester screening
• Those at lowest risk of <1:1500 receive negative screening test results and have no further testing is done.
Assuming that women accept diagnostic testing when informed that the risk is elevated, detection approaches 91 percent.
18.
NON-INVASIVE PRENATAL TESTING
•CfDNA screening can be performed at any time after 9 to 10 weeks gestation ( 1st trimester
screening)
• CfDNA has the highest sensitivity and specifcity of any aneuploidy screening test.
• Detection rate of 99% for trisomy 21 and 98% for trisomy 18 with false positive rate as
<1%
• Since cfDNA screening has a PPV far higher than other screening, it may be offered as a
secondary screening test for
• women who wish to avoid amniocentesis.
• CfDNA screening is most commonly used to screen for autosomal trisomies—trisomy 21,
trisomy 18, and trisomy13, 45,X (Turner syndrome), 47,XXX, 47,XXY, and 47,XYY, trisomies 16
and 22, specifc microdeletion syndromes
• If the cfDNA screening test is positive or yields a no-call I.e. no results , additional genetic
counselling is indicated, and amniocentesis should be offered.
19.
PRENATAL GENETIC DIAGNOSTICTEST
Diagnostic testing will confirm or exclude a suspected diagnosis of chromosomal abnormality.
Most of the diagnostic tests are invasive and carry a risk of miscarriage.
I. CHORIONIC VILLUS SAMPLING
CVS is usually performed between 11 wk to 13 wk 6days of gestation, with cells obtained from chorion
Frundosum under ultrasound guidance for karyotyping.
Detection rate being 99%.
INDICATION:
• Abnormal early genetic screening on a non-invasive prenatal screening, first trimester combined screening,
or abnormalities on ultrasound.
• Previous autosomal trisomic foetus
• Women or partner has a chromosomal abnormalities or are carriers of chromosomal inversions
• Repeated first trimester abortions
20.
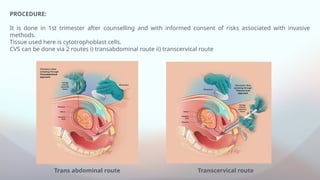
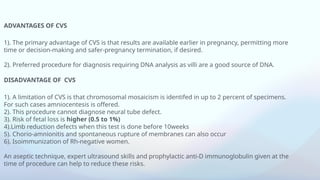
Trans abdominal routeTranscervical route
PROCEDURE:
It is done in 1st trimester after counselling and with informed consent of risks associated with invasive
methods.
Tissue used here is cytotrophoblast cells.
CVS can be done via 2 routes i) transabdominal route ii) transcervical route
21.
ADVANTAGES OF CVS
1).The primary advantage of CVS is that results are available earlier in pregnancy, permitting more
time or decision-making and safer-pregnancy termination, if desired.
2). Preferred procedure for diagnosis requiring DNA analysis as villi are a good source of DNA.
DISADVANTAGE OF CVS
1). A limitation of CVS is that chromosomal mosaicism is identifed in up to 2 percent of specimens.
For such cases amniocentesis is offered.
2). This procedure cannot diagnose neural tube defect.
3). Risk of fetal loss is higher (0.5 to 1%)
4).Limb reduction defects when this test is done before 10weeks
5). Chorio-amnionitis and spontaneous rupture of membranes can also occur
6). Isoimmunization of Rh-negative women.
An aseptic technique, expert ultrasound skills and prophylactic anti-D immunoglobulin given at the
time of procedure can help to reduce these risks.
22.
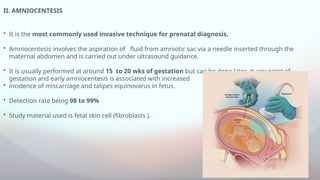
II. AMNIOCENTESIS
• Itis the most commonly used invasive technique for prenatal diagnosis.
• Amniocentesis involves the aspiration of fluid from amniotic sac via a needle inserted through the
maternal abdomen and is carried out under ultrasound guidance.
• It is usually performed at around 15 to 20 wks of gestation but can be done later at any point of
gestation and early amniocentesis is associated with increased
• incidence of miscarriage and talipes equinovarus in fetus.
• Detection rate being 98 to 99%
• Study material used is fetal skin cell (fibroblasts ).
23.
INDICATIONS
1. Diagnosis ofgenetic disorders. The main indication for amniocentesis is for foetal
karyotyping for an increased risk of aneuploidy like-
(i) Women with positive serum screening for Down's syndrome.
(ii) Women of advanced maternal age (traditionally > 35 years)
(iii) Ultrasound detection of an abnormality or soft tissue markers.
(iv) Parental balanced translocation
(v) A previous history of chromosomal abnormality.
2. Diagnosis of inborn errors of metabolism like cystic fibrosis.
3. Diagnosis of infection, e.g. cytomegalovirus infection.
DISADVANTAGE
4. Fetal loss rate 0.1 to 0.3%
5. Amniotic fluid leaking
6. Vagina spotting
24.
III. CORDOCENTESIS ORFETAL BLOOD SAMPLING OR PERCUTANEOUS UMBILICAL BLOOD
SAMPLING
• It was initially described for fetal transfusion of red blood cells in the setting of anemia from
alloimmunization and fetal anemia assessment remains the most common indication.
• Other indications include -
1. assessment and treatment of platelet alloimmunization
2. for fetal karyotype determination, particularly in cases of mosaicism identifed following
amniocentesis or CVS
3. drug delivery.
• Improvements in testing using an amniocentesis specimen have eliminated the need for fetal blood
sampling in most cases.
• Fetal blood sampling is often performed near the placental cord insertion site, where it may be
easier to enter the cord if the placenta lies anteriorly. Alternatively, a free loop of cord may be
punctured.
25.
COMPLICATIONS:
• Higher riskof fetal loss is seen in this method approximately to
1%.
• Deceleration of fetal heart sound as umbilical cord can go into
spasm.
• Fetomaternal haemorrhage
• Abruptio placenta
• Preterm labour
• Trauma to mother’s intestine or vessels
Cordocentesis
26.
IV. FETOSCOPY
The introductionof small fibre optic scope into the amniotic cavity under ultrasound guidance allows
direct visualisation of Foetus for biopsy or surgery.
V. FOETAL TISSUE BIOPSY
Fetal tissue biopsy is done under ultrasound or Fetoscopic guidance from specific tissue for diagnosis
of pathological conditions.
This procedure has high incidence of miscarriage and preterm delivery.
VI. PLACENTAL BIOPSY
It can be performed transvaginally up to 13 weeks and transabdominally after 13 weeks under
Ultrasound guidance.
VII. PREIMPLANTATION GENETIC DIAGNOSIS
This technique employs the analysis of oocyte or embryo before conception. This can be done by polar
body analysis.
27.
FETAL MRI
Fetal MRIscanning (non invasive method ) can now be undertaken to clarify the presence of some
abnormalities.
This is particularly useful following the identification of brain abnormalities on ultrasound.
The identification of CNS abnormalities is very Gestation dependent and therefore it may not on
reassurance to a couple until the third trimester .