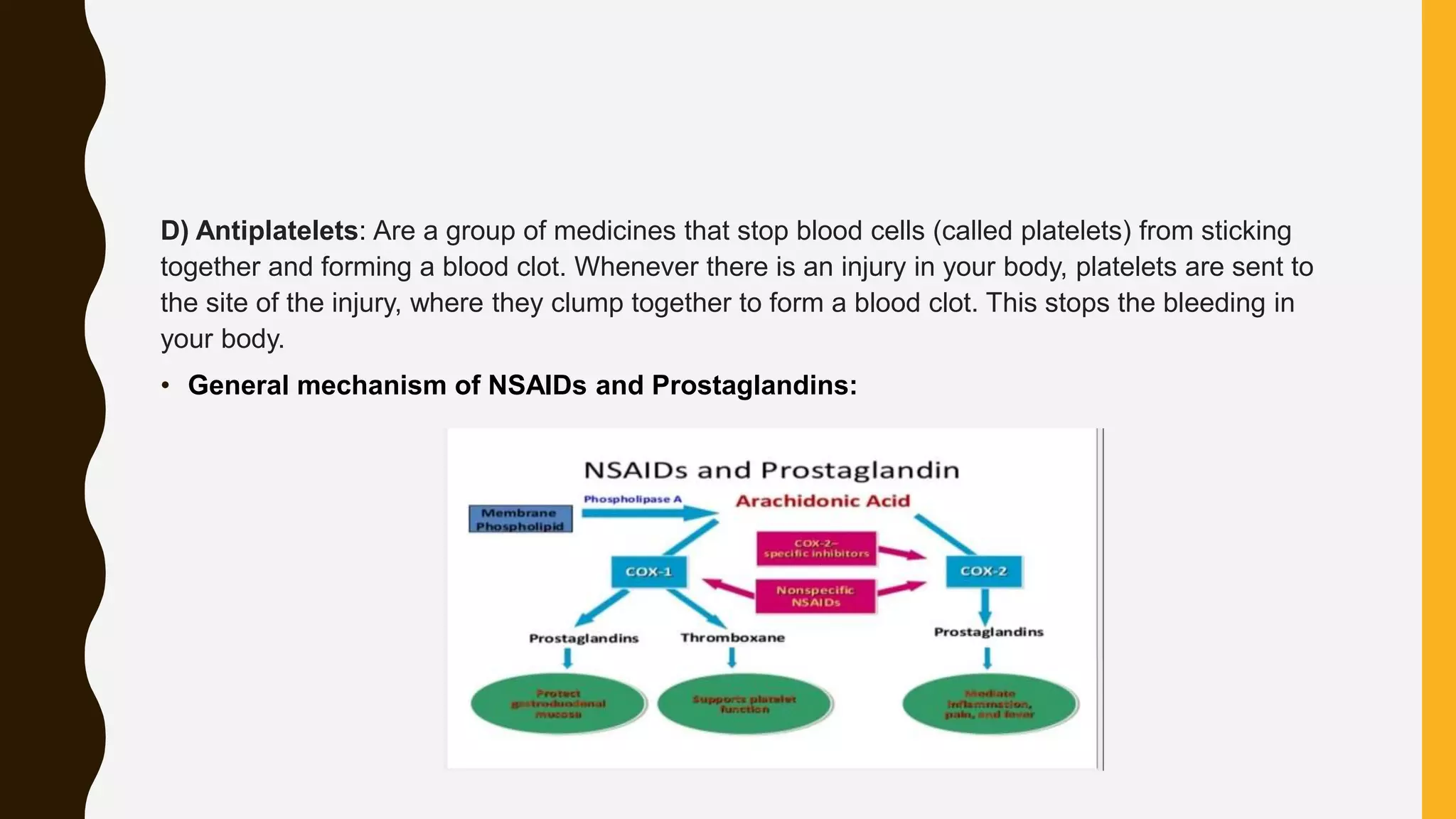
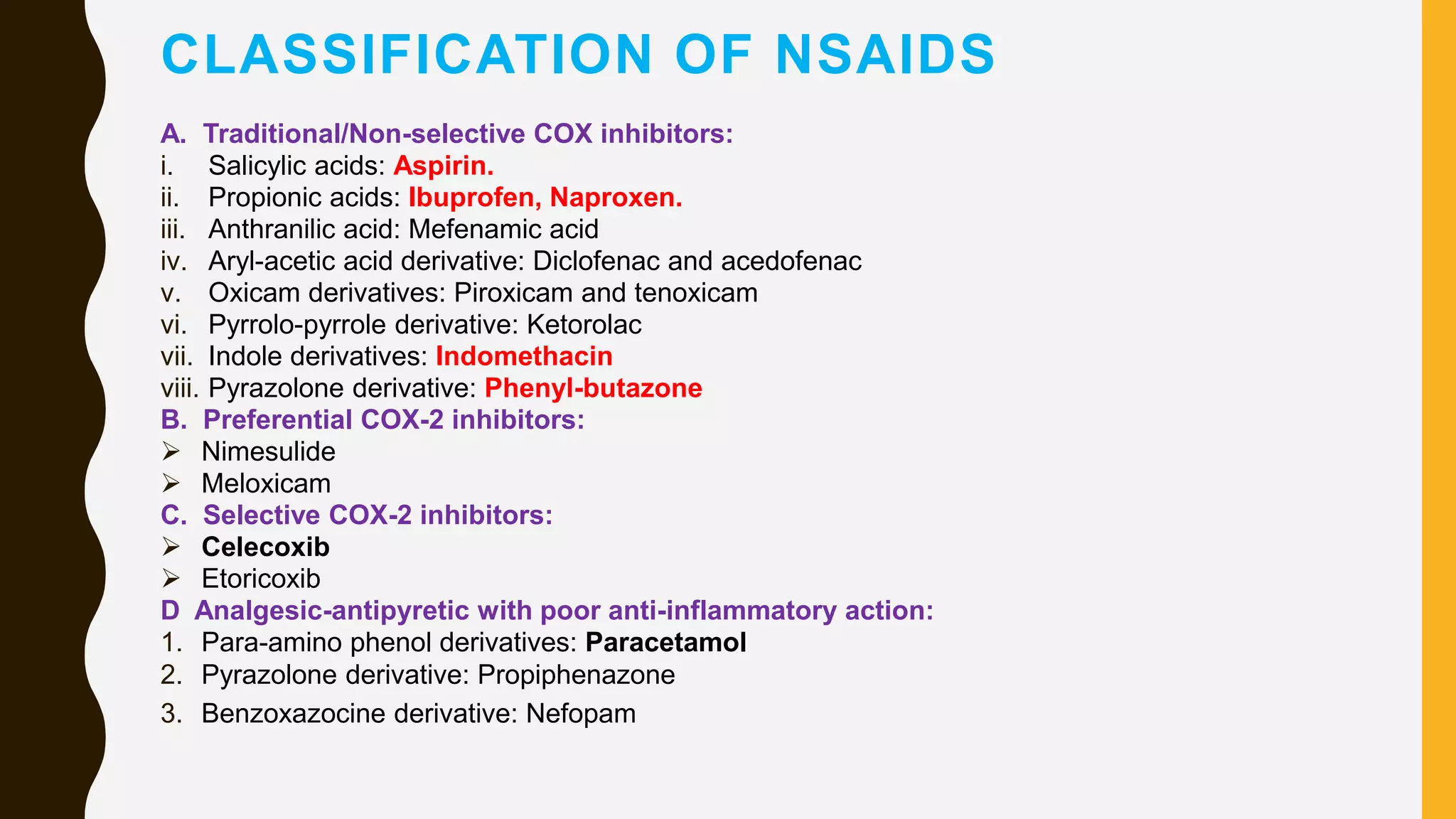
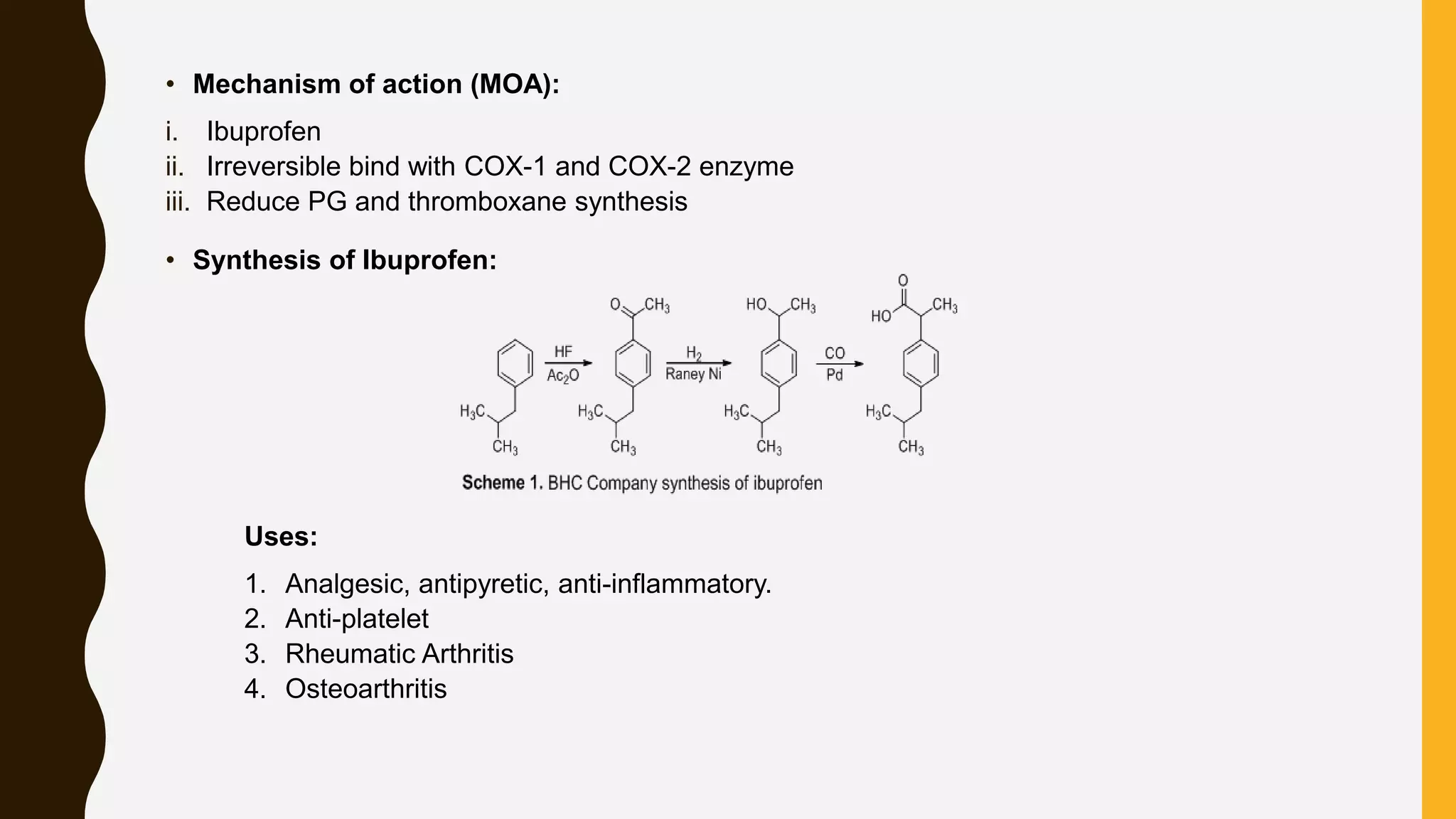
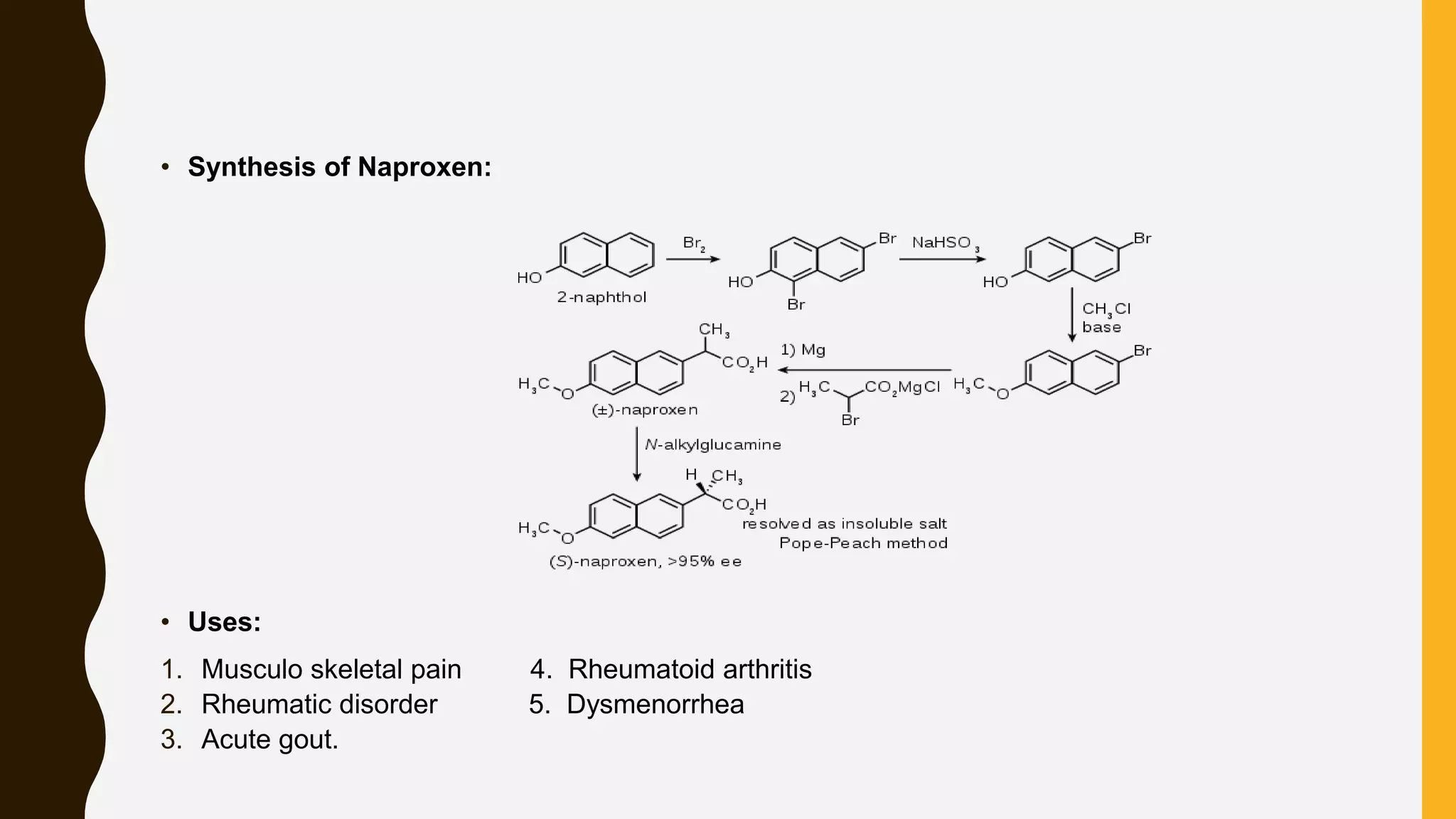
Nonsteroidal anti-inflammatory drugs (NSAIDs) are a class of medications used to reduce pain, inflammation, and fever, including categories such as analgesics, antipyretics, anti-inflammatories, and antiplatelets. Common NSAIDs include aspirin, ibuprofen, and naproxen, each having specific mechanisms of action and therapeutic uses. The document outlines the classification, structure-activity relationships, mechanisms of action, and synthesis processes for several NSAIDs.




















![ANTI HYPERTENSIVE AGENTS [MEDICINAL CHEMISTRY] BY P.RAVISANKAR, HYPERTENSION,...](https://cdn.slidesharecdn.com/ss_thumbnails/antihypertensiveagents-ravi-130615193634-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)














































































