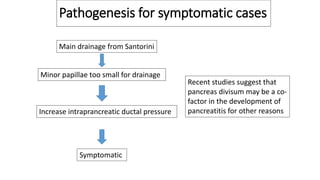
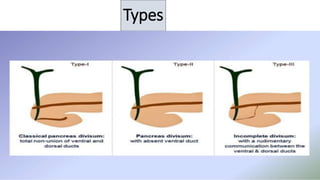
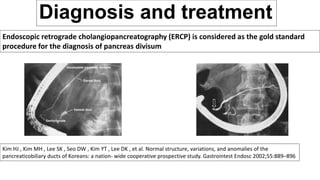
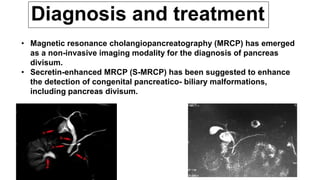
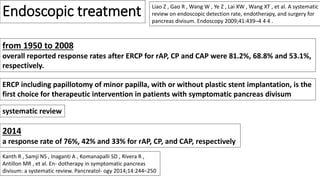
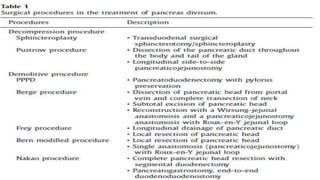
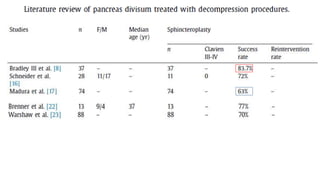
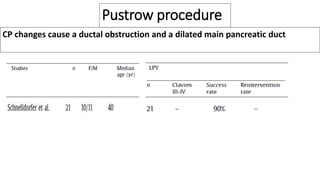
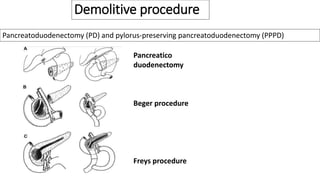
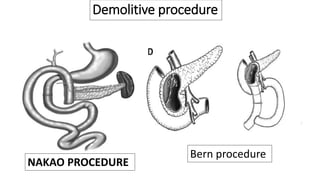
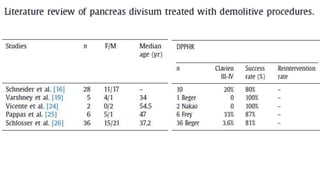
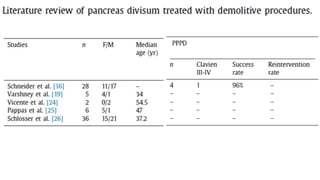
This document discusses pancreas divisum, a congenital anomaly where the pancreas does not fully fuse during development. It has a 5% incidence rate but only 5% of those are symptomatic. Symptomatic cases are due to increased pressure from drainage through the smaller Santorini duct rather than the main duct. Diagnosis is via ERCP or MRCP. Treatment options include endoscopic procedures like sphincterotomy of the minor papilla or surgery if endoscopy fails. Surgical options range from sphincteroplasty to reconstruct the drainage pathway to more extensive resections like pancreaticoduodenectomy.















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





