Mucor poster

A 54 year old female, with history of uncontrolled Diabetes Mellitus presented with complaints of progressively severe frontal headaches with associated nausea and dizziness. CT scan of the head revealed a 10 cm frontal bone lytic lesion extending into the nasal bones with evidence of sequestrum. Mucosal thickening and opacification of the frontal sphenoid and ethmoid sinuses was also noted. MRI was consistent with CT finding and revealed further cortical destruction of frontal calvarium outer table along with para-meningeal and dural enhancement. CSF studies were negative. Patient was started on intravenous antifungal therapy with Amphotericin B lipid complex. Frontal sinus trephination with irrigation/aspiration and simultaneous diagnostic nasal endoscopy revealed no frank pus or necrosis. Aspirate’s bacterial and fungal culture were negative. Patient underwent an open incision trephination of frontal sinus that revealed destruction/moth-eaten appearance of the anterior table of the frontal sinus, biopsies were taken, No pus was encountered.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Mucor poster
Similar to Mucor poster (20)
Mucor poster
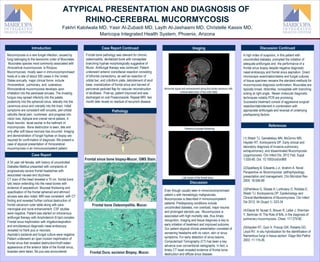
- 1. ATYPICAL PRESENTATION AND DIAGNOSIS OF RHINO-CEREBRAL MUCORMYCOSIS Fakhri Kalolwala MD, Yasir Al-Zubaidi MD, Layth Al-Jashaami MD, Christelle Kassis MD, Maricopa Integrated Health System, Phoenix, Arizona Introduction Mucormycosis is a rare fungal infection, caused by fungi belonging to the taxonomic order of Mucorales. Mucorales species most commonly associated with rhinocerbral mucormycosis is Rizopus. Mucormycosis mostly seen in immunocompromised hosts at a rate of about 500 cases in the United States annually. major clinical forms include rhinocerebral, pulmonary, and cutaneous. Rhinocerebral mucormycosis develops upon inhalation into the paranasal sinuses. The invading fungus may spread inferiorly into the palate, posteriorly into the sphenoid sinus, laterally into the cavernous sinus and cranially into the brain. Initial symptoms are consistent with sinusitis, peri-orbital cellulitis /facial pain, numbness and progress into vision loss, diplopia and cranial nerve palsies. A black necrotic facial eschar is the hallmark of mucomycosis. Bone destruction is seen, late and only after soft tissue necrosis has occurred. Imaging and demonstration of fungal hyphae on biopsy are required for confirmation of diagnosis. We present a case of atypical presentation of rhinocerebral mucormycosis in an immunocompetent patient. Case Report Frontal bone pathology was relevant for chronic osteomyelitis, devitalized bone with nonseptate branching hyphae morphologically suggestive of Mucor. Antifungal therapy was continued. Patient underwent anterior craniofacial resection consisting of bifrontal craniectomy, as well as resection of orbital bar, and cribriform plate, debridement of skull base, cranialization of frontal sinus and harvest of pericranial pedicled flap for vascular reconstruction of skullbase. Post-op, patient improved and was discharged on oral Posaconazole. Repeat MRI two month later reveal no residual of recurrent disease. Case Report Continued References A 54 year old female, with history of uncontrolled Diabetes Mellitus presented with complaints of progressively severe frontal headaches with associated nausea and dizziness. CT scan of the head revealed a 10 cm frontal bone lytic lesion extending into the nasal bones with evidence of sequestrum. Mucosal thickening and opacification of the frontal sphenoid and ethmoid sinuses was also noted. MRI was consistent with CT finding and revealed further cortical destruction of frontal calvarium outer table along with para- meningeal and dural enhancement. CSF studies were negative. Patient was started on intravenous antifungal therapy with Amphotericin B lipid complex. Frontal sinus trephination with irrigation/aspiration and simultaneous diagnostic nasal endoscopy revealed no frank pus or necrosis. Aspirate’s bacterial and fungal culture were negative. Patient underwent an open incision trephination of frontal sinus that revealed destruction/moth-eaten appearance of the anterior table of the frontal sinus, biopsies were taken, No pus was encountered. Discussion A high index of suspicion, in this patient with uncontrolled diabetes, prompted the initiation of adequate antifungals and the performance of a frontal sinus biopsy despite negative diagnostic nasal endoscopy and frontal sinus aspiration. Direct microscopic examination/stains and fungal cultures of tissue specimen remains the standard methods for mucormycosis diagnosis confirmation. Mucorales are typically broad, ribbonlike, nonseptate with branching arising at right angle. Newer molecular diagnostic techniques notably PCR are promising. Successful treatment consist of aggressive surgical resection/debridement in combination with appropriate antifungals and reversal of underlying predisposing factors. (1) Walsh TJ, Gameletsou MN, McGinnic MR, Hayden RT, Kontoyiannis DP. Early clinical and laboratory diagnosis of invasive pulmonary, extrapulmonary, and disseminated Mucormycosis (zygomycosis). Clin Infect Dis. 2012 Feb; Suppl 1:S55-60. Doi: 10.1093/cid/cir868 (2)Spellberg B, Edwards J Jr, Ibrahim A. Novel Perspective on Mucormycosis: pathophysiology, presentation and management. Clin Microbiol Rev 2005: 18:556-69 (3)Petrikkos G, Skiada A, Lortholary O, Roilides E, Walsh TJ, Kontoyiannis DP. Epidemiology and Clinical Manifestations of Mucormycosis, Clin Infect Dis 2012; 54 (Suppl 1): S23-34 (4)Glazer M, Nusair S, Breuer R, Lafair J, Sherman Y, Berkman N. The Role of BAL in the diagnosis of pulmonary mucormycosis. Chest: 117:279-82 (5)Hayden RT, Quin X, Procop GW, Roberts GD, Lloyd RV. In situ hybridization for the identification of filamentous fungi in tissue section. Diagn Mol Pathol 2002; 11:119-26. Even though usually seen in immunocompromised patient s with hematologic malignancies, Mucomycosis is described in immonocompetent patients. Predisposing conditions include uncontrolled diabetes, iron overload, major trauma and prolonged steroids use. Mucormycosis is associated with high mortality rate, thus timely recognition, imaging and tissue diagnosis is key to early initiation of treatment and improved outcome. Our patient atypical clinical presentation consisted of worsening headache with no vision, skin or sinus symptoms. For early detection of sinus lesions, Computerized Tomography (CT) has been a key advance over conventional radiographs. In fact, a timely CT head revealed evidence of frontal bone destruction and diffuse sinus disease. Pathology Discussion ContinuedImaging Abnormal signal and enhancement along the frontal calvarium with cortical destruction of the outer table Lytic lesion of the frontal bone Pansinus mucosal thickening Frontal sinus bone biopsy-Mucor, GMS Stain. Frontal bone Osteomyelitis. Mucor. Frontal Dura, excision Biopsy, Mucor.