Surgical anatomy of osteomeatal complex
•Download as PPTX, PDF•
179 likes•52,373 views

osteomeatal complex

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Surgical anatomy of osteomeatal complex
Similar to Surgical anatomy of osteomeatal complex (20)
Recently uploaded
Recently uploaded (20)
Surgical anatomy of osteomeatal complex
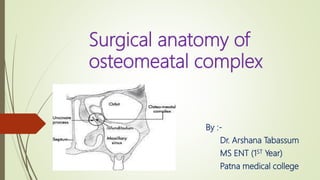
- 1. Surgical anatomy of osteomeatal complex By :- Dr. Arshana Tabassum MS ENT (1ST Year) Patna medical college
- 2. CONTENTS Definition Boundaries Parts of OMC Anterior and posterior OMC Anatomical variations
- 3. Osteomeatal complex Also known as ostiomeatal unit or key area or critical area It is final common pathway for drainage and ventilation of ethmoid, maxillary and frontal sinuses.
- 4. Osteomeatal complex contd….. It is a functional concept rather than an anatomic structure with defined boundaries. Goal of naming this area is to emphasize the concept that inflammation in OMC can lead to anatomic and functional obstruction of anterior sinuses. Any of these cells, clefts, ostia, recesses or cavities may be affected by a pathological process, thereby contributing to the symptoms and pathophysiology of sinusitis. Medical and surgical strategies are devised to eliminate OMC obstruction and restore sinonasal function. For performing FESS the knowledge of OMC anatomy is also very important.
- 5. Boundaries . When the middle turbinate is reflected medially, the borders and components can be more readily appreciated. Anteriorly, the unit is in open communication with the anterior nasal cavity. The agger nasi and atrium of the middle meatus also have an anterosuperior, and anterior (respectively) relations to the complex. Superiorly, the ostiomeatal complex (OMC) is limited by the basal lamella.
- 6. Posteriorly, The basal lamella continues along the length of the middle turbinate and consequently forms the posterior border of the space. Inferiorly, the ostiomeatal unit has an open communication with the middle meatus. The drained contents of the unit will travel in the meatus along with the superior border of the inferior concha, which forms the floor of the middle meatus. Medially, the complex is limited by the body of the middle concha. Laterally, the lamina papyracea of the ethmoid sinuses borders the complex.
- 8. The ostiomeatal complex is differently defined by several authors. Naumann H ..he was the first to develop this anatomical unit and coined the term term osteometal complex. According to him it consists of semilunar hiatus and middle meatus. Scribano et al. have defined the ostiomeatal complex as a complex including the maxillary sinus ostium, ethmoid infundibulum and middle meatus; in other words, as the final site of drainage from the frontal and maxillary sinuses and anterior ethmoidal cells. Casiano has defined the ostiomeatal complex as the ethmoid bulla, uncinate process and adjacent spaces and ostia draining the anterior sinuses (anterior ethmoid sinus, frontal and maxillary sinuses).
- 9. Laine & Smoker have defined the ostiomeatal complex as an aerated channel of the middle meatus representing the final common pathway for drainage of the maxillary and frontal sinuses and anterior ethmoid cells, delimited by the uncinate process, ethmoidal bulla and middle turbinate. Shankar et al. have defined ostiomeatal complex as a complex including the maxillary ostium, ethmoid infundibulum, hiatus semilunaris, middle meatus, frontal recess, ethmoid bulla and uncinate process. Stammberger & Kennedy , defining ostiomeatal complex as a functional unit of the anterior ethmoid complex representing the final common pathway for drainage and ventilation of the frontal, maxillary and anterior ethmoid cells.
- 10. The ostiomeatal complex is composed of five structures: maxillary ostium: drainage channel of the maxillary sinus infundibulum: common channel that drains the ostia of the maxillary antrum and anterior ethmoid air cells to the hiatus semilunaris
- 11. ethmoid bulla: usually a single air cell that projects over the hiatus semilunaris uncinate process: hook-like process that arises from the posteromedial aspect of the nasolacrimal duct and forms the anterior boundary of the hiatus semilunaris hiatus semilunaris: final drainage passage; a region between the ethmoid bulla superiorly and free-edge of the uncinate process
- 12. Showing the Osteomeatal complex (OMC)-(a) The OMC-small compartment located in the region between the middle turbinate and the lateral nasal wall in the middle meatus-represents the key region for the drainage for the maxillary, anterior ethmoid and frontal sinuses
- 13. Some authors divide this osteomeatal complex into anterior and posterior. Space infront of basal lamella is anterior osteomeatal complex, while the space behind the basal lamella of middle turbinate containing the posterior ethmoidal cells is referred to as the posterior ethmoidal complex, thus recognising the importance of basal lamella as an anatomical landmark to the posterior ethmoidal system. the anterior and the posterior osteomeatal complex has separate drainage systems. So when the disease is limited to the anterior compartment of the osteomeatal complex, the ethmoid cells can be opened and diseased tissue removed as far as the basal lamella, leaving the basal lamella undisturbed minimising the risk during surgery.
- 17. Common anatomical variations of the OMC concha bullosa paradoxical middle turbinate, uncinate process hypertrophy and pneumatization, hypertrophy of the bulla ethmoidalis and the agger nasi cell presence of the maxilo-ethmoidal cell (Haller’s cell)
- 18. Concha Bullosa & paradoxical middle turbinate The middle turbinate may be congenitally filled with air (pneumatized). This variation is referred as a concha bullosa. Also, there are also instances where the middle turbinate develops in a sigmoid shape – with a superior convexity and an inferior concavity. This condition is referred to as a paradoxical middle turbinate.
- 20. Uncinate process deviation The uncinate process may deviate from its typical posteroinferior course and arise in a medial fashion that obstructs the middle meatus and the ethmoid infundibulum. In cases where hypoplastic maxillary sinuses are present, lateral elevation of the uncinate process until it fuses with the medial orbital wall can impede the integrity of the orbit.
- 21. Based on the ethmoid bulla’s configuration and size and the orientation of the uncinated process, the abnormalities in OMC are classified into six types Earwaker defined that as follows: type 1: vertical UP orientation and enlarged or prolapsed ethmoid bulla, type 2: vertical UP orientation and normal ethmoid bulla, type 3: vertical UP orientation and absent or hypoplastic ethmoid bulla, type 4: horizantal UP orientation and enlarged or prolapsed ethmoid bulla, type 5: horizantal UP orientation and normal ethmoid bulla, type 6: horizantal UP orientation and absent or hypoplastic ethmoid bulla UP orientation ethmoid bulla Type 1 Vertical enlarged or prolapsed Type 2 Vertical Normal Type 3 Vertical absent or hypoplastic Type 4 Horizantal enlarged or prolapsed Type 5 Horizantal Normal Type 6 Horizantal absent or hypoplastic
- 22. A 20-year-old male with type 1 UP insertion. Coronal CT scan shows that UP is attached (straight arrow) to the laminae papyracea (asteriks) on the left. A 38-year-old male with type 2 UP insertion. (A, B) Two consecutive cross-sections on coronal CT. Left uncinate process is attached (A, arrow) to the posterior agger nasi cell (B, arrow)
- 23. The superior attachment of the uncinate process have implications on drainage of frontal sinuses. If attached to skull base middle turbinate If attaches laterally to orbit ___ drains into superior aspect of infundibulum drains medial to uncinate process into middle meatus
- 24. Curved tip of UP The UP can show a set of rotation and attachment variations. The most commonly observed variation is a medially oriented UP. If it moves anteriorly and exits from the middle meatus, it is called ‘Kaufmann’s double middle turbinate’. The horizontal and vertical orientation of UP is determined by adjacent structures: ethmoid bulla affecting frontal OMU drainage and middle concha. Horizontal UP is always related to an enlarged ethmoid bulla. The UP can also take the form of a hook or can be pneumatized.
- 25. A 41-year-old female with horizontal and vertical UP. (A) The horizontal orientation of the left uncinate process (straight arrow) is accompanied by a large ethmoid bulla (dotted arrow) on the coronal CT. (B) In a different case, both uncinate processes seem to be localized vertically.
- 26. The aeration of UP is called uncinate bulla. Even though the mechanism of occurrence is not sufficiently known, it is predicted that the agger nasi cells stem from the growth of the UP’s frontmost and uppermost section towards the inside. The uncinate bulla are considered to be a variation that can alter the ventilation through the infidibulum, anterior ethmoid cells and frontal recess. It increases the wideness of the uncinate, so it constitutes to be potentially dangerous for the infundibulum. Narrowness in the infundibulum is of clinical significance, since it can disrupt ventilation in the frontal ethmoid cells and the frontal recess region. It can cause significant deterioration in OMU function by acting functionally like a concha bullosa or a widened ethmoid bulla. As it is in the uncinate bulla and haller cells, the pathological effect should be considered in cases where the number of combinations of anatomical variations is higher. Uncinate bulla
- 27. A 44-year-old female with uncinate bulla. (A) Coronal CT image shows that both uncinate processes are pneumatized (straight arrow). (B) In a different case, bilateral uncinate bulla variation (straight arrow) causes significant narrowing in the ostiomeatal unit.
- 28. Bifid UP A 23-year-old male with bifid uncinate process. Coronal CT demonstrates (A) bilateral and (B) right-sided bifid UP (straight arrow) in different cases.
- 29. Atelectatic UP Sometimes, UP’s free end shows hypoplastic development and attaches to orbital medial wall inferior section of lamina paprisea. This condition is called atelectatic UP . Generally, it is seen together with an opacified hypoplastic maxillary sinus . This variation is very important in the cases where anterior endoscopic sinus surgery is applied. If it is not defined radiologically, it can cause important complications posing a great danger for the orbital and optic nerve during unsinectomy. •NCBI •NCBI A 52-year-old male with atelectatic uncinate process. Opacified hypoplastic maxillary sinus antrum (dotted arrow) is shown together with UP (straight arrow) attached to the inferomedial orbital wall on coronal CT image.
- 30. Hypertrophy of the Bulla Ethmoidalis and the Agger Nasi Cell Ethmoid bulla is large anterior ethmoid air cells found in many people The degree of pneumatization may be highly variable, from a giant ethmoid bulla that pushes the UP medially. Enlarged ethmoid bulla includes cells that grow up to the ethmoid ceiling superiorly, basal lamella of the middle concha posteriorly, and lamina paprisea laterally. The relationship of ethmoid bulla with lamina papyracea and lateral, and the relationship of frontal cranial fossa in superior with base should be clarified in preoperative CT. Ethmoid bulla is a reliable surgery marker point because it is the highest and the most constant anterior ethmoid cell.
- 31. The giant ethmoid bulla may enlarge to narrow or obstruct the middle meatus and infundibulum
- 34. Blood supply ___ mainly by anterior ethmoidal artery which is the branch of ophthalmic artery ( br of internal carotid artery) Venous drainage _____mainly by anterior ethmoidal vein.
- 35. Thank you