Download as PDF, PPTX


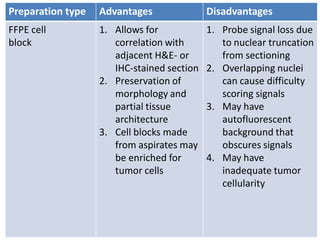
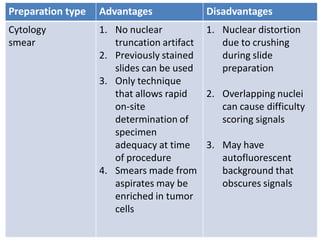
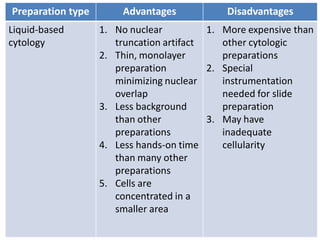
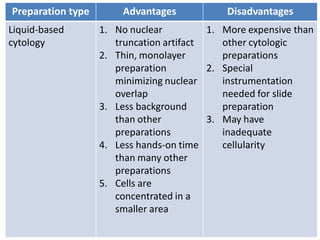
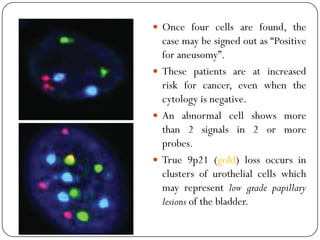
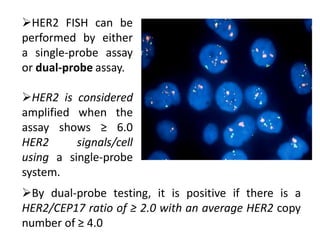
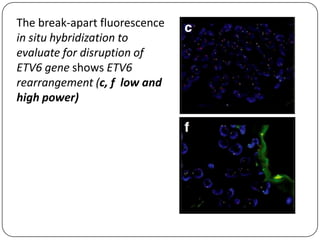



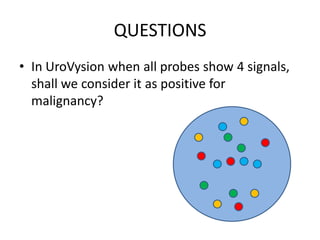

Molecular testing techniques can be used on cytology specimens to facilitate cancer patient management. Fluorescence in situ hybridization (FISH) is well-suited for detecting genomic abnormalities in cytology specimens. FISH involves hybridizing fluorescent probes to target sequences to visualize locations. It can detect gains, losses, amplifications, and rearrangements. A variety of cytology specimens can be used for FISH, including smears, cell blocks, and liquid-based preparations. FISH has applications in detecting abnormalities in cancers like urothelial carcinoma, breast cancer, and lymphoma.























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

















