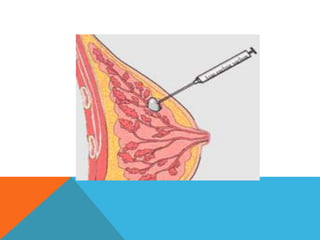
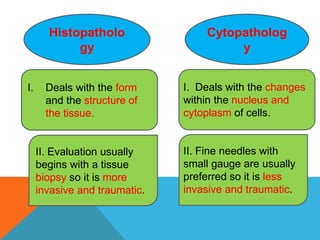
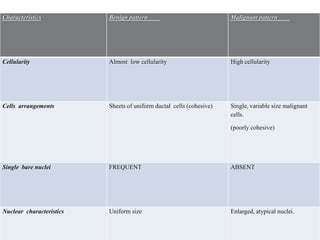
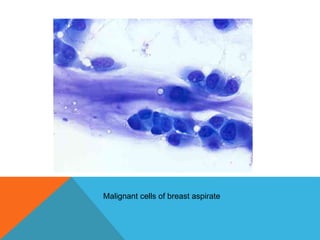
The document provides a comprehensive overview of cytopathology, defining it as the study of individual cells to identify diseases, and contrasting it with histopathology, which examines intact tissues. It discusses various sampling techniques (exfoliative, abrasive, and fine needle aspiration) and their respective advantages and disadvantages, including faster and less invasive procedures in cytopathology. Additionally, the document outlines the diagnostic utility of cytopathology in differentiating benign and malignant lesions, as well as monitoring treatment responses.




































































![Semen Analysis.lab .ppt [Compatibility Mode].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/semenanalysis-240326105510-ec373892-thumbnail.jpg?width=640&height=640&fit=bounds)
























