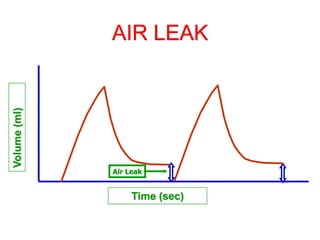
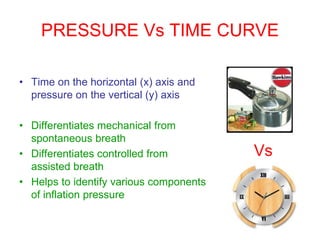
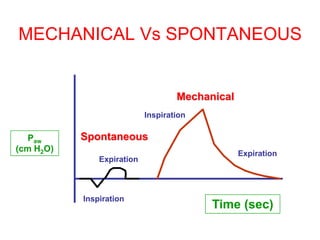
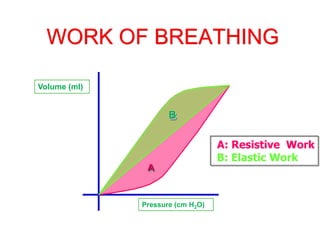
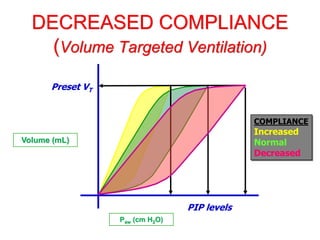
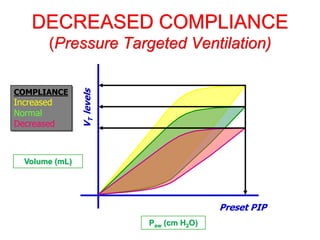
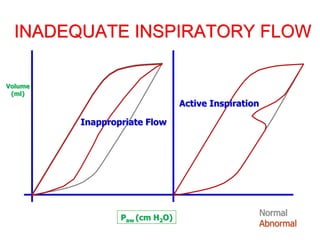
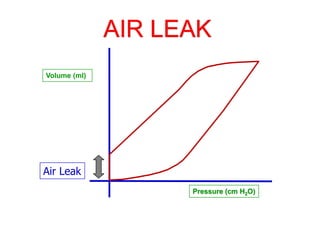
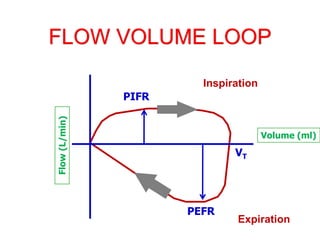
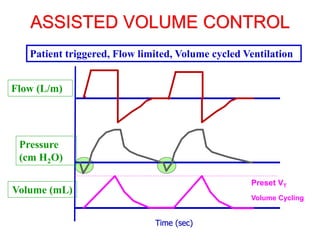
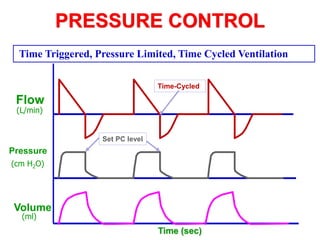
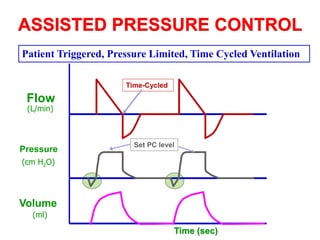
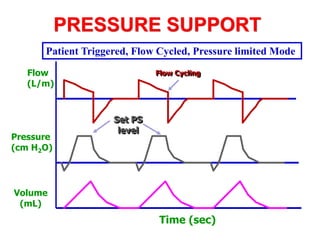
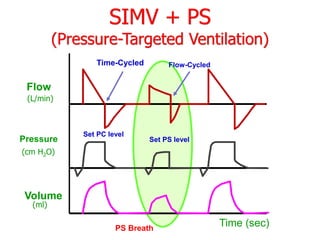
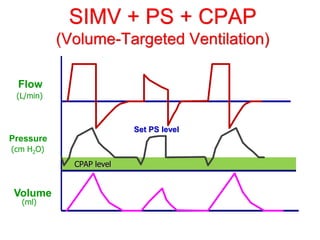
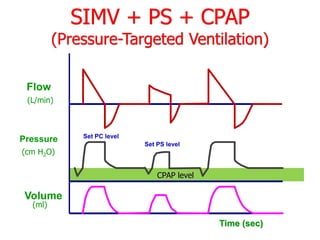
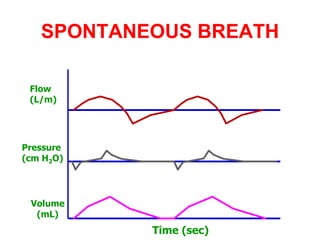
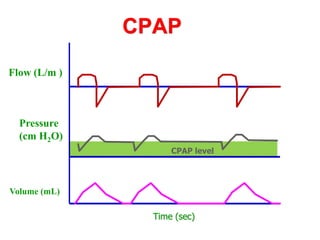
This document provides an overview of mechanical ventilation graphics including scalars like flow/time, pressure/time and volume/time curves as well as loops like pressure/volume and flow/volume. It describes the normal components and appearances of these graphics as well as how they can be used to identify the mode of ventilation, abnormalities related to compliance, resistance and leaks, and the patient's work of breathing. The graphics provide more detailed information than numbers alone and help clinicians recognize normal patterns and abnormalities.




























![Mechanical ventilation[1]](https://cdn.slidesharecdn.com/ss_thumbnails/mechanicalventilation1-150109002450-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)













![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








