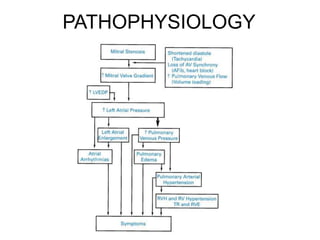
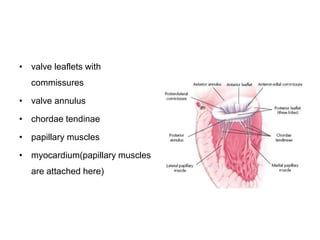
Mitral stenosis is characterized by obstruction of the left ventricular inflow tract at the mitral valve due to structural abnormalities of the valve. Rheumatic fever is the leading cause of mitral stenosis. Classical symptoms include fatigue, dyspnea, cough, and leg swelling. On examination, findings include a low volume pulse, diastolic murmur, and enlarged liver. Complications include atrial fibrillation, pulmonary hypertension, heart failure, and thromboembolism.