
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Aortic valve disease
Similar to Aortic valve disease (20)
More from DR NIKUNJ SHEKHADA
More from DR NIKUNJ SHEKHADA (20)
Recently uploaded
Recently uploaded (20)
Aortic valve disease
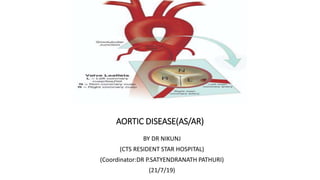
- 1. AORTIC DISEASE(AS/AR) BY DR NIKUNJ (CTS RESIDENT STAR HOSPITAL) (Coordinator:DR P.SATYENDRANATH PATHURI) (21/7/19)
- 2. ANATOMY • The aortic valve is the last of four cardiac valves through which the blood is pumped before it goes to the rest of the body. • It separates the left ventricular outflow tract from the aorta. • Its main function is to prevent backward blood flow from the aorta to the left ventricle, while allowing the blood to flow forward during systole with minimal resistance.
- 4. AORTIC ROOT • The aortic root is the anatomic segment between the left ventricle and the ascending aorta. It contains the aortic valve and other anatomic elements, which function as a unit. The aortic root has several anatomic components: • subcommissural triangles, • aortic annulus, • aortic cusps, • aortic sinuses or sinuses of Valsalva, • sinotubular junction.
- 6. THE SUBCOMMISSURAL TRIANGLES • The subcommissural triangles are part of the left ventricular out fow tract, • The subcommissural triangles of the noncoronary aortic cusp are fibrous extension of the intervalvular fibrous body and membranous septum, whereas the subcommissural triangle beneath the left and the right aortic cusps is an extension of the muscular interventricular septum.
- 7. THE AORTIC ANNULUS • The aortic annulus, a fibrous structure with a scalloped shape, attaches the aortic valve to the left ventricle. • It is attached directly to the myocardium in approximately 45% of its circumference, and to fibrous structures in the remaining 55% • The diameter of the aortic annulus is 10% to 20% larger than the diameter of the sinotubular junction of the aortic root in young patients . As the number of elastic fibers in the arterial wall decreases with age, the sinotubular junction dilates, and its diameter tends to become equal to that of the aortic annulus in older patients.
- 8. • With dilation of the aortic annulus, the subcommissural triangles of the noncoronary cusp tend to become more obtuse as the crescent shape of the aortic annulus along its fibrous insertion flattens.
- 11. CUSPS • The normal aortic valve has three cusps. Each cusp has a semilunar shape and has a base and a free margin. The base is attached to the aortic annulus in a crescent fashion. The point at which the free margin of a cusp joins its base is the commissure, and • the ridge in the aortic wall that lies immediately above the commissures is the sinotubular junction. • At the mid point of each free edge is fibrou nodulus arantii on either side of nodulus is extremely thin. • The free margin of an aortic cusp extends from one of its commissures to the other. The length of the free margin of an aortic cusp is approximately 1.5 times the length of its base.
- 12. CUSPS • The three aortic cusps often have different sizes in a person, and the right and noncoronary cusps are usually larger than the left cusp. • The same cusp may have different sizes in individuals with the same body surface area • During diastole, the free margins and part of the body of the three cusps touch each other approximately in the center of the aortic root to seal the aortic orifice. • Thus, the average length of the free margins of three aortic cusps must exceed the diameter of the sinotubular junction to allow the cusps to coapt centrally and render the aortic valve competent .
- 13. • The aortic leaflets display three layers of connective tissue: the ventriculosa on the ventricular side, the fibrosa on the aortic side, and the spongiosa between them • The fibrosa is mainly composed of collagen fibers while the ventriculosa mostly consists of elastic fibers. • Between these two layers, the spongiosa is composed of a mucopolysaccharide gel-like substance that facilitates the motion of the ventriculosa and fibrosa.
- 14. • If a pathologic process causes shortening of the length of the free margin of a cusp, or if the sinotubular junction dilates, the cusps cannot coapt centrally, resulting in aortic insufciency . • If the length of a free margin is elongated, the cusp prolapses, and depending on the degree of prolapse, aortic insufficiency
- 16. AORTIC SINUSES, OR SINUSES OF VALSALVA • The spaces contained between the aortic annulus and the sinotubular junction are the aortic sinuses. There are three cusps and three sinuses: • left cusp and sinus, • right cusp and sinus, • noncoronary cusp and sinus. • The left main coronary artery arises from the left aortic sinus, and the right coronary artery arises from the right aortic sinus. • There are three sinuses of the aortic valve, each related to the valve’s corresponding cusps. Each sinus is divided into three areas a central part and two adjacent parts, which are named according to the valve cusps they adjoin. • The noncoronary sinus is also refferred to as the posterior aortic sinus.
- 17. AORTIC SINUSES, OR SINUSES OF VALSALVA • The aortic sinuses facilitate closure of the aortic valve by creating eddies and currents between the cusps and arterial wall . • They also prevent the cusps from occluding the coronary artery orifices during systole, thus guaranteeing myocardial perfusion during the entire cardiac cycle.
- 18. RIGHT CORONARY SINUS • entire right coronary sinus lies adjacent to the RVOT. • central part lies adjacent to the crista supraventricularis, • left part is adjacent to the area of the RVOT in the angle between the crista supraventricularis and the pulmonary valve. • posterior (noncoronary) part of the right coronary sinus is related to the area of the right ventricle posteroinferior to the crista supraventricularis. • Inferiorly, the entire right coronary sinus is related to the interventricular septum; the muscular septum lies under the central and left parts, while either membranous or muscular septum may lie under the posterior part of the right coronary sinus.
- 19. NONCORONARY SINUS • The atrialchambers with the intervening atrial septum lie adjacent to the noncoronary sinus. • right and central parts of the noncoronary sinus are related to the right atrium and the interatrial septum, • left part is related to the left atrium. • Inferiorly, the right part, like the posterior part of the right coronary sinus, may be related either to the membranous or the muscular septum depending on the size of the membranous septum. However, beneath the central part of the noncoronary sinus, the membranous septum is a constant structure. The left part of the noncoronary sinus inserts into the anterior mitral leaflet
- 20. LEFT CORONARY SINUS • posterior part of the left coronary • it is related to the left atrium posteriorly and to the anterior mitral leaflet inferiorly. • central part of the left aortic sinus is the only part of the aortic root that is not related to a cardiac chamber; it is adjacent to the epicardium only. • right part of the left coronary sinus lies adjacent to the pulmonary trunk at the level of the left pulmonary sinus. inferior to it lies the muscular interventricular septum.
- 21. • The aortic root of young individuals is elastic and very compliant. It expands and contracts during the cardiac cycle. • The normal aortic root has a fairly consistent shape, and the sizes of the cusps, the aortic annulus, the aortic sinuses, and the sinotubular junction are somewhat interdependent. • Thus, large cusps have a proportionally large annulus, sinus, and sinotubular junction.
- 23. AORTIC STENOSIS Epidemiology and Etiology • Isolated aortic stenosis (AS) is more common in men than in women and is found in 2% of people 65 years of age and older. • The most common causes of AS include agerelated calcific degeneration, bicuspid aortic valve, and rheumatic aortic valve. • The distribution of these causes varies across age groups and geographic regions. • Age related degeneration is the most common cause of AS in patients older than 70 years. • In contrast, bicuspid aortic valve calcification accounts for most surgical cases in patients younger than 70 years.
- 24. • Valvular AS has three principle causes 1. Congenital bicuspid valve with superimposed calcification 2. Calcification of normal trileaflet valve 3. Rhumatic disease.
- 25. • Fixed obstruction to LVOT may occur above the valve(supravalvular stenosis) • Below the valve (subvalvular stenosis)
- 26. CONGENITAL BICUSPID VALVE WITH SUPERIMPOSED CALCIFICATION • Congenital malformation can be • Unicuspid: infancy • Bicuspid : • Ttricuspid : • Domeshaped diaphragm:
- 27. CALCIFIC AORTIC VALVE DISEASE • Calcific aortic valve disease affecting a congenital bicuspid or normal trileaflet valve is the most commone cause of AS in adults
- 29. RHEUMATIC AORTIC STENOSIS • It Results from adhesions and fusion of the comissures and cusps and vasclarazation of the leaflets of the valve ring • Leading to retraction and stiffening of the free borders of the cusps • Calcific nodules deveope on bothe surface and orifice is reduced to small round or triangular opening. • It can be regurgitant as well as stenotic.
- 31. PATHOPHYSIOLOGY • No appreciable gradient exists across the normal aortic valve during systole. • In AS, gradual obstruction of the left ventricular outflow leads to an increased left ventricular afterload and left ventricular wall stress, elevated left ventricular systolic and diastolic pressures, decreased aortic pressure, and prolonged left ventricular ejection time. • Over time, this results in compensatory concentric left ventricular hypertrophy (LVH) to maintain ejection fraction. • In patients with chronic severe AS, this compensatory mechanism may become insufficient, leading to gradual dilation and thinning of the left ventricle, and result in a decrease in ejection fraction and in congestive heart failure.
- 32. PATHOPHYSIOLOGY • Myocardial oxygen supply and demand is also altered in AS. • LVH, increased systolic pressure, and prolonged ejection time result in increased myocardial oxygen demand. • Increased diastolic pressure and prolonged systolic ejection time result in decreased diastolic and myocardial perfusion time and hence myocardial oxygen supply. • The alteration in myocardial oxygen supply and demand is the underlying mechanism behind myocardial ischemia in patients with AS, even in the absence of coronary artery disease.
- 33. SYMPTOMS • The classic symptoms of AS are angina, exertional syncope, and symptoms of congestive heart failure such as shortness of breath. • Angina: frequent symptom of pt with svere AS • Syncope: reduced cerebral perfusion. • GI Bleeding
- 34. PHYSICAL EXAMINATION • palpation of carotid upstroke(Slow rising late peaking,low amplitude) • Evaluation of systolic murmur • Assessment of splitting of second heart sound • Signs of HF • crescendo-decrescendo systolic ejection murmur heard best at the second right intercostal space, which may variably radiate to the carotid arteries. • A palpable thrill may be present in severe cases of AS. • Palpation of the arterial pulse may reveal a weak and delayed pulse known as pulsus parvus et tardus.
- 35. DIAGNOSIS AND GRADING • Two-dimensional transthoracic echocardiography is the most common modality for the diagnosis and grading of AS
- 36. • X ray chest • EKG • CARDIAC CT • CARDIAC CATHETERIZATION • TMT
- 37. NATURAL HISTORY • Without intervention, • Multiple studies consistently reported survivals of 3 years for angina and syncope • 1.5 to 2 years for dyspnea and heart failure. • These findings have driven recommendations for early surgical intervention in patients with symptomatic AS. • One third of asymptomatic patients with severe AS will become symptomatic in 2 years with an estimated cardiac death of less than 1% each year to 5% each year. • Patients with higher grades of AS severity seem to progress at a faster rate than lower grades of AS. • After AS becomes moderate, aortic valve area decreases on average by 0.1 cm2 per year, the pressure gradient across the valve rises on average by 7 mm Hg per year, and the jet velocity increases by 0.3 m/sec per year.
- 38. AORTIC REGURGITATION • disturbance in any of the components of the functional unit of the aortic valve (e.g., cusps, sinuses of Valsalva, sinotubular junction, ventriculoaortic junction). • In general, the causes can be divided into • affect the valve cusps (e.g., calcific degeneration, congenitally bicuspid valve, infective endocarditis, rheumatic disease, myxomatous degeneration) • affect the aortic root (e.g., aortic dissection, aortitis of various etiologies such as syphilis, connective tissue disorders such as Marfan syndrome) Primary Valve disease Primary Root disease Congenital (bicuspid aortic valve) Rheumatic fever Infective endocarditis ,Collagen vascular diseases ,Degenerative aortic valve disease Myxomatous (prolapse) Traumatic Longstanding, uncontrolled hypertension Marfan syndrome ,Idiopathic aortic dilation Cystic medial necrosis, Senile aortic ectasia and dilation Aortic dissection, Marfan's syndrome Syphilitic aortitis Giant cell arteritis, Takayasu arteritis, Ankylosing spondylitis, Whipple disease
- 40. THE PATHOPHYSIOLOGY OF AR • dependent on the acuity of onset and duration of the disease process. • ACUTE AR, typically caused by aortic dissection, infective endocarditis, trauma, or valve prosthesis failure, there is a sudden increase in left ventricular end-diastolic volume because of the regurgitation. • Since the left ventricle has limited compliance and does not have time to adapt, the left ventricular end- diastolic pressure (LVEDP) rises rapidly
- 41. • CHRONIC AR, there is a slow and insidious progression of left ventricular (LV) dilation and eccentric hypertrophy because of an increase in left ventricular end-diastolic volume, LVEDP, and wall stress. • Dilation of the LV, while maintaining normal systolic function, increases total stroke volume and maintains forward flow. • This increase in stroke volume coupled with an increase in LVEDP is associated with the wide pulse pressure typical of chronic AR. • Eventually, the hypertrophic response is exhausted, and LVEF drops as afterload increases, leading to heart failure and its associated clinical presentation.
- 44. Valve Dysfunctions Valve Dysfunctions corresponding Lesions Lesions Type I: Normal leaflet motion Annular dilatation Leaflet perforation Vegetation Type II: Leaflet prolapse Leaflet rupture, distension Commissure detachment Type IlIa: Restricted leaflet closure and opening Leaflet thickening Commissure fusion Calcification Type Illb: Restricted leaflet closure only Sino-tubular dilatation
- 45. CLINICAL FEATURES • ACUTE AR :usually exhibit sudden or rapidly progressive cardiovascular collapse, which can be life threatening if not addressed promptly. • They often exhibit ischemic symptoms because of the decrease in coronary blood flow and increased myocardial oxygen demand. • CHRONIC AR : asymptomatic for a long period of time because of the compensatory LV changes. • Once the compensatory response is exhausted, the patients start having heart failure symptoms 1. PALPITATION - early symptom 2. HEAD POUNDING - on exertion 3. EXERTIONAL DYSPNOEA 4. ORTHOPNOEA 5. PAROXYSMAL NOCTURNAL DYSPNOEA 6. EXCESSIVE DIAPHORESIS 7. ANGINA - on exertion/ at rest - nocturnal 8. CCF - late
- 46. PULSE IN AR • Corrigan’s pulse or • Water hammer pulse or • Collapsing pulse - Rapid rise and rapid fall • Bisferiens’s pulse -two peaks in systole • A pulse that is bounding and forceful, rapidly increasing and subsequently collapsing, it resembles the strike of waterhammer
- 47. • S1- may be soft due to premature closure of the mitral valve. • A2 –normal or accentuated when AR is due to aortic root disease. • S2- absent or single or exhibit narrow or paradoxical splitting • S3 GALLOP - due to increased LV end diastolic volume or impaired LV function • Systolic ejection sound - related to abrupt distention of the aorta by the augmented stroke volume.
- 48. • CHRONIC AORTIC REGURGITATION • Early diastolic murmur • High pitched, blowing decrescendo Best heard in the 3rd left intercostal space with the patient sitting up and leaning forward breath held in forced expiration • Aortic root disorders murmur is best heard along right sternal border musical murmur Longer the duration of murmur severer the aortic regurgitation • Becomes short - cardiac failure • Austin flint murmur • Soft, low pitched rumbling mid diastolic murmur. • Diastolic displacement of the anterior leaflet of the mitral valve by the aortic regurgitation stream.
- 49. • Classic signs of widened pulse pressure may also be found, including 1. Corrigan or water-hammer pulse, 2. De Musset sign (bobbing of the head with heart beats), 3. Quincke pulse (pulsations of the lip and fingers), 4. Traube sign (pistol shot sounds over the femoral artery), 5. Müller sign (pulsations of the uvula). 6. Becker sign - Visible systolic pulsations of the retinal arterioles 7. Light-house sign – Alternate flushing & blanching of forehead 8. Landolfi’s sign - Change in pupil size with each systole 9. Gerhardt’s sign - Visible systolic pulsations of spleen 10. Rosenbach’s sign - Visible systolic pulsations of liver 11. Corrigan’s sign – Dancing carotid in neck 12. Hill sign: Popliteal cuff systolic pressure exceeding brachial cuff systolic pressure by more than 20 mmHg.
- 50. DIAGNOSTIC CRITERIA • Transthoracic echocardiography with Doppler colorflow is the most useful tool for the diagnosis of AR. • The jet width and vena contracta width on Doppler color-flow are used to qualitatively assess the severity of AR, whereas the regurgitant volume, regurgitant fraction, and regurgitant orifice area are used for the quantitative assessment.
- 54. CHEST X RAY • acute AR, there may be minimal cardiac enlargement, but marked enlargement is a common finding in chronic AR.
- 55. ECG •LV hypertrophy •Left axis deviation •Left atrial enlargement •LV volume overload pattern - Prominent Q waves in leads I, aVL, and V3 to V6 and relatively small R waves in V1
- 56. • AORTIC ANGIOGRAPHY 1. Mild (1+) - A small amount of contrast enters the LV during diastole and clears with each systole 2. Moderate AR (2+) - Contrast enters the LV with each diastole, but the LV chamber is less dense than the aorta 3. Moderately severe AR (3+) - The LV chamber is equal in density to the ascending aorta. 4. Severe AR (4+) - Complete, dense opacification of the LV chamber occurs on the first beat, and the LV is more densely opacified than the ascending aorta • CARDIAC MRI :CMR provides accurate measurements of regurgitant volumes and the regurgitant orifice in AR. It is the most accurate noninvasive technique for assessing LV end systolic volume, diastolic volume, and mass
- 57. CARDIAC CATHETERIZATION • Class I indications for cardiac catheterization under current ACC/AHA guidelines: • Assessment of coronary anatomy prior to aortic valve surgery in patients with risk factors for coronary artery disease • Assessment of severity of AR, LV function, or aortic root size when noninvasive tests are inconclusive or are discordant with clinical findings.