Downloaded 12 times


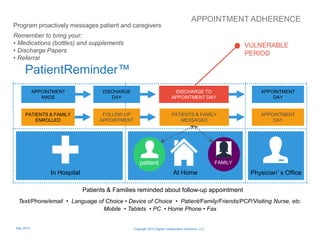
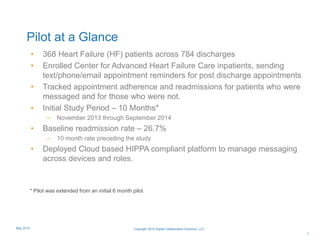
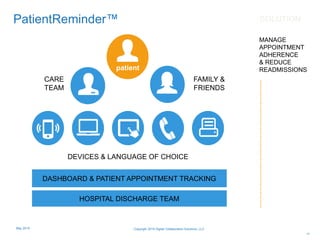
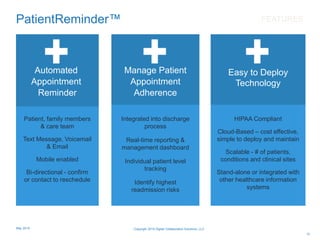

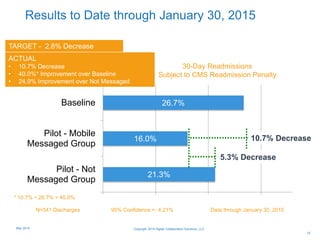
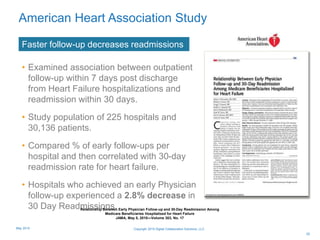
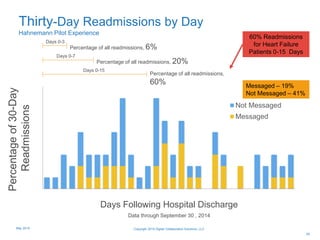
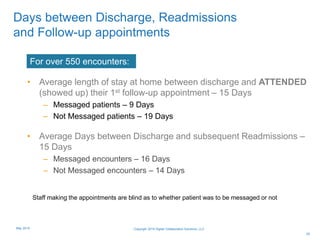
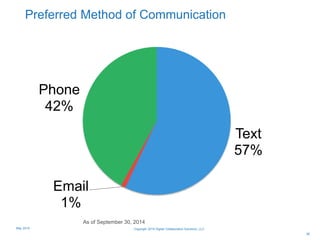
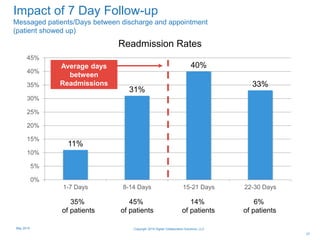
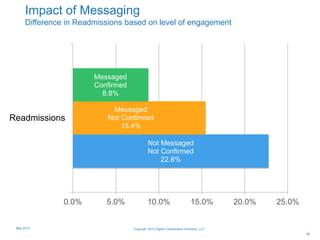
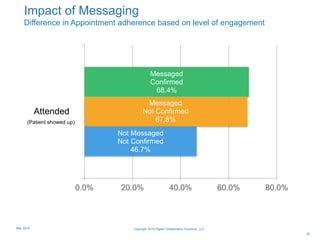
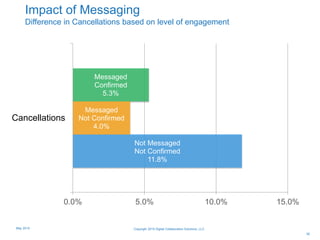
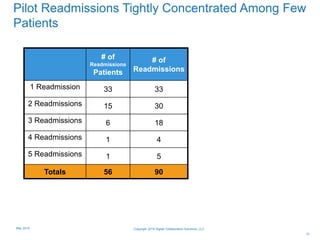
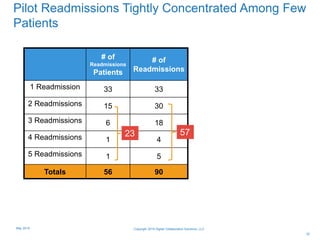
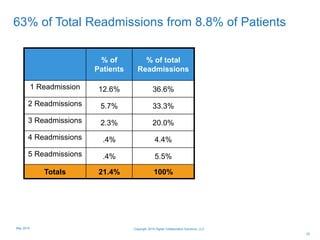
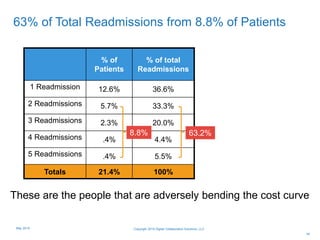
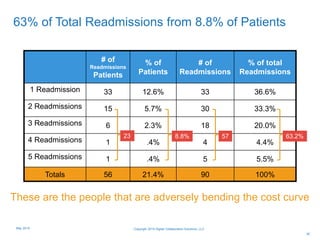
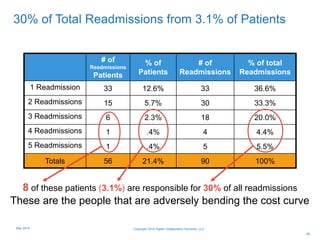
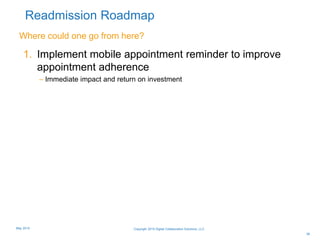
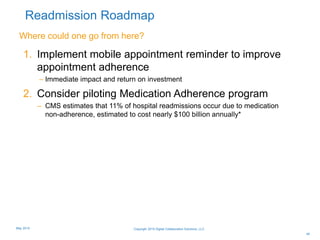
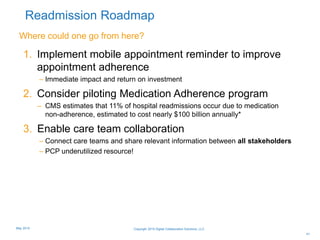
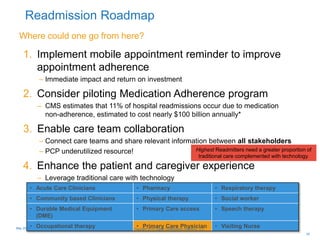
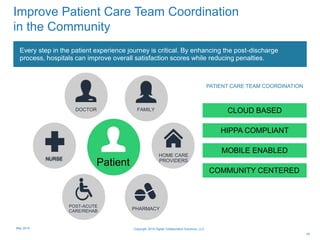


The document discusses the implementation of a mobile health (mHealth) initiative aimed at improving patient engagement and reducing 30-day readmission rates through appointment reminders sent via text, email, or phone. A pilot program involving heart failure patients demonstrated a 10.7% decrease in readmissions and highlighted the importance of follow-up care in preventing rehospitalization. The findings indicate that effective communication and reminders can enhance patient adherence to follow-up appointments and contribute to better health outcomes.



















![Va pcmh study 6 2014[1]](https://cdn.slidesharecdn.com/ss_thumbnails/vapcmhstudy620141-140801153322-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)














![Pagina web[1]](https://cdn.slidesharecdn.com/ss_thumbnails/paginaweb1-100927194701-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





























































