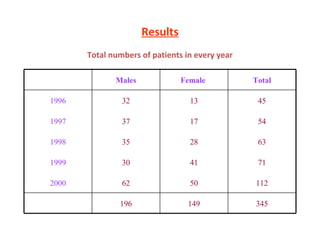
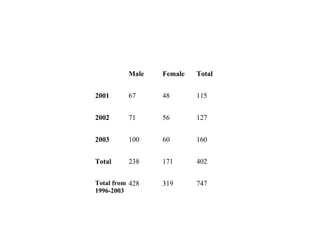
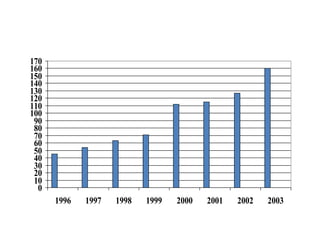
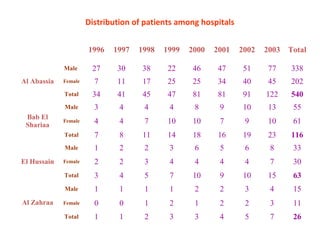
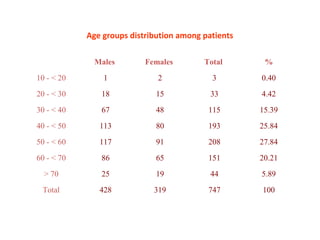
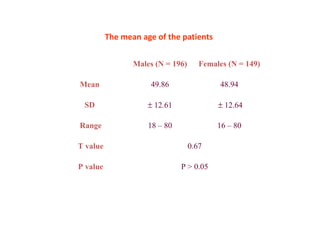
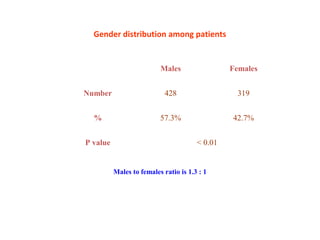
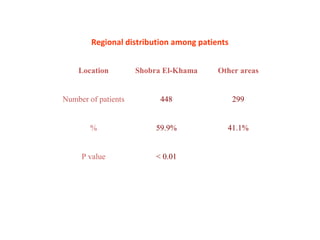
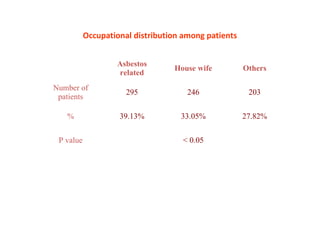
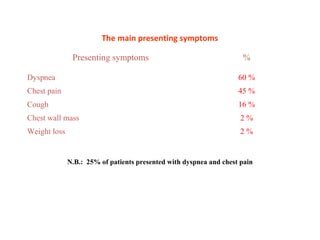
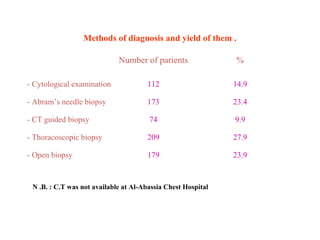
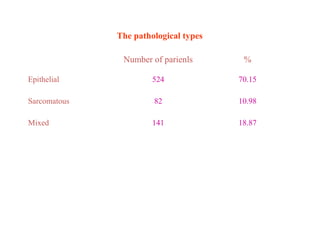
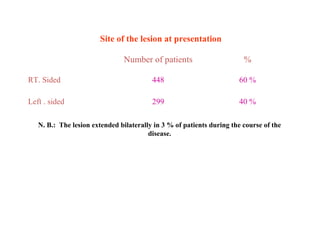
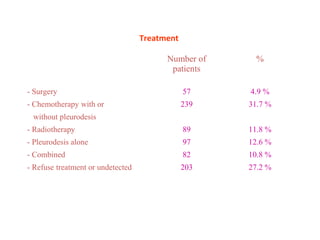
This study analyzed 747 cases of malignant pleural mesothelioma diagnosed between 1996-2003 at hospitals in Egypt. Most patients were males between 40-60 years old living in industrial areas. The main presenting symptoms were dyspnea and chest pain. Asbestos exposure was identified as the primary risk factor. Diagnosis was typically made via biopsy and patients had poor prognosis, surviving on average 12 months after diagnosis. The study concluded that mesothelioma is increasing in Egypt likely due to asbestos exposure and recommended preventative measures to reduce asbestos pollution.