Download to read offline
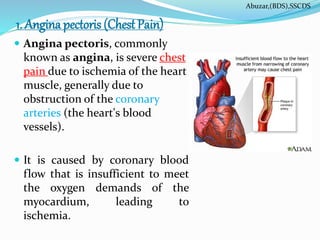
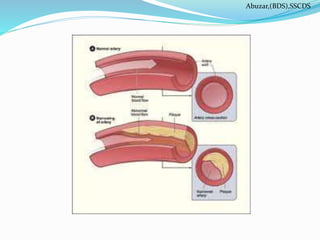
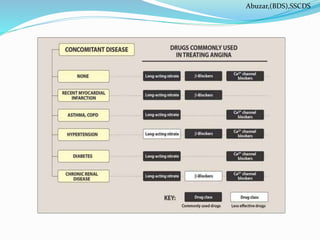


This document discusses angina pectoris (chest pain), including its causes, types, risk factors, and treatment. It begins by defining angina as chest pain due to temporary heart muscle ischemia, usually due to coronary artery obstruction. It describes the three main types of angina - stable, unstable, and mixed forms. The major risk factors for angina are then listed. The document focuses on drug therapies for angina, explaining the mechanisms and effects of the three main classes: organic nitrates, beta-blockers, and calcium channel blockers. Specific drugs like nitroglycerin and nifedipine are discussed in terms of their pharmacokinetics, mechanisms of action, and adverse effects in treating an












































![Anti-angina_F.K.ppt_for_midwife[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anti-anginaf-230902073731-f0ce562d-thumbnail.jpg?width=640&height=640&fit=bounds)






















