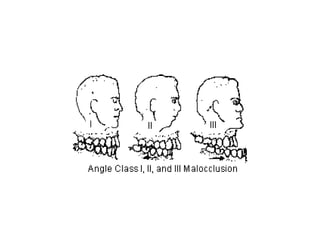
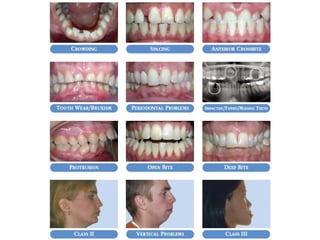

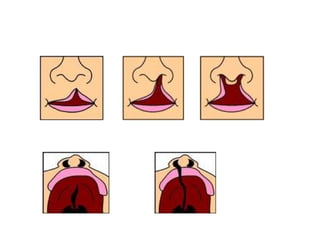
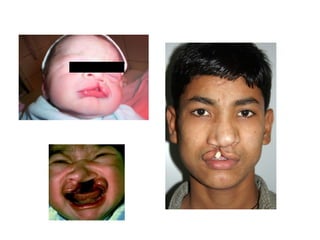
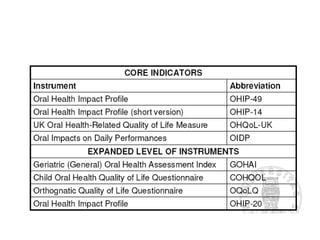

This document discusses methods for measuring various oral health conditions in epidemiology. It covers malocclusion measurement tools like Angle's classification and the Index of Orthodontic Treatment Need (IOTN). For oral cancer, it discusses prevalence, survival rates, and risk factors. Cleft lip and palate occurrence is expressed as proportions or rates. Quality of life measures like the Oral Health Impact Profile (OHIP) and General Oral Health Assessment Index (GOHAI) are presented.























































































