Download to read offline



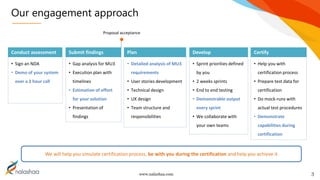
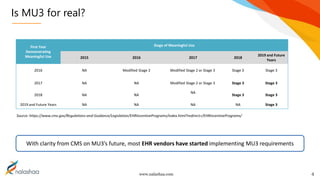


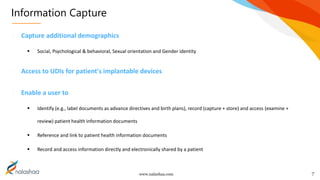



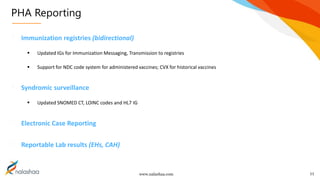
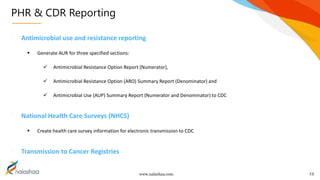
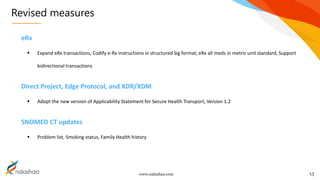


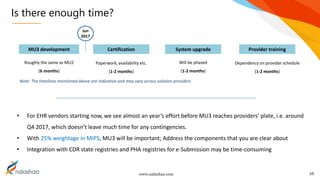


The document outlines the Meaningful Use Stage 3 (MU3) implementation by a software services company specializing in technology solutions. It discusses various requirements and changes associated with MU3, including data capture, application access, and reporting changes, emphasizing the need for a collaborative approach for certification. Finally, it addresses the effort required for compliance and the timeline implications for EHR vendors as they prepare for MU3 adoption.


































![Trudel cms-rules-072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudel-cms-rules-0728101-100810094307-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel Cms Rules 072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudelcmsrules0728101-12814484645456-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel Cms Rules 072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudelcmsrules0728101-12814485135294-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel Cms Rules 072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudelcmsrules0728101-12814486180502-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel cms-rules-072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudel-cms-rules-0728101-100810090601-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel Cms Rules 072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudelcmsrules0728101-12814488066912-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel cms-rules-072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudel-cms-rules-0728101-100810090705-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








