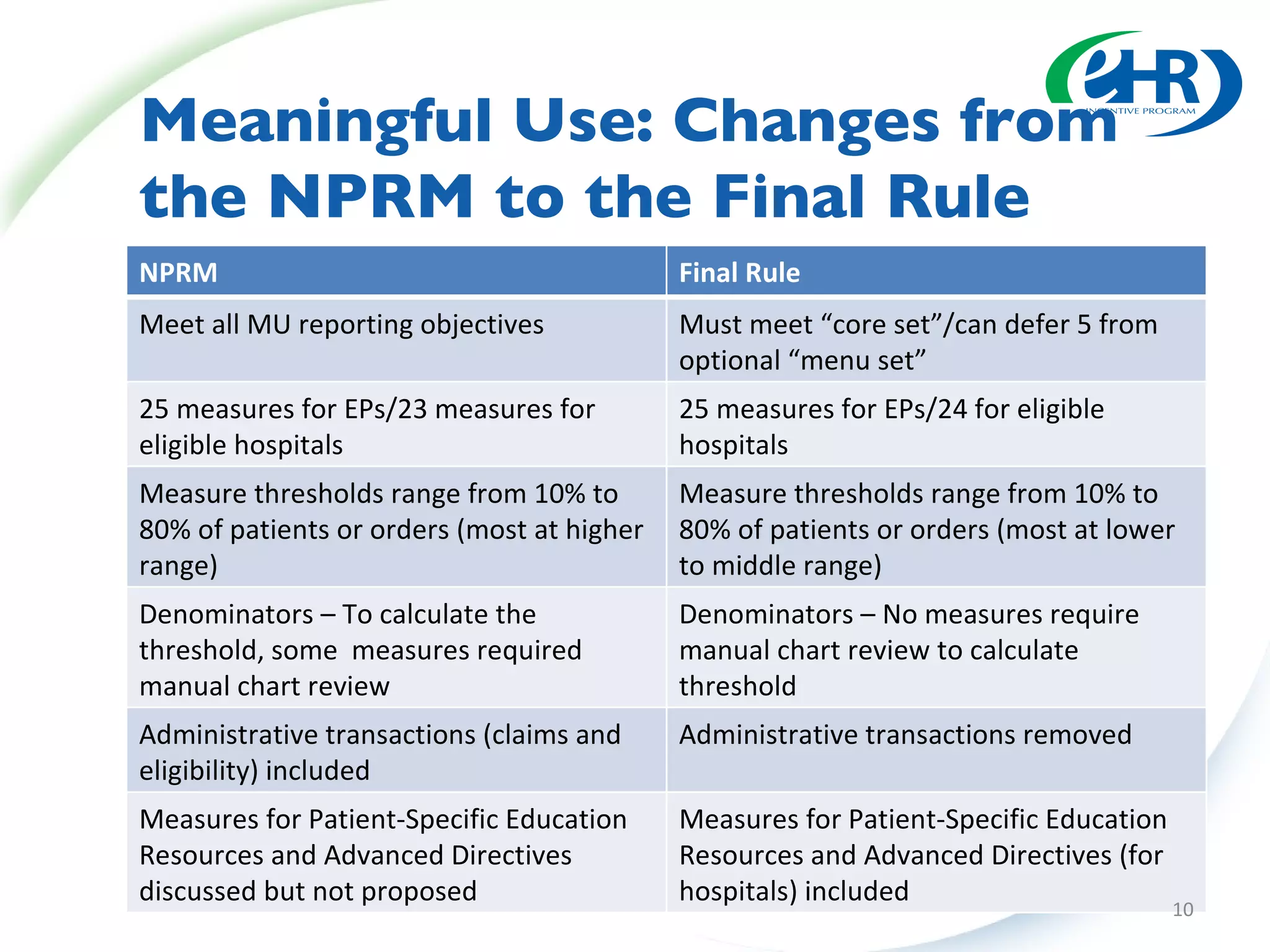
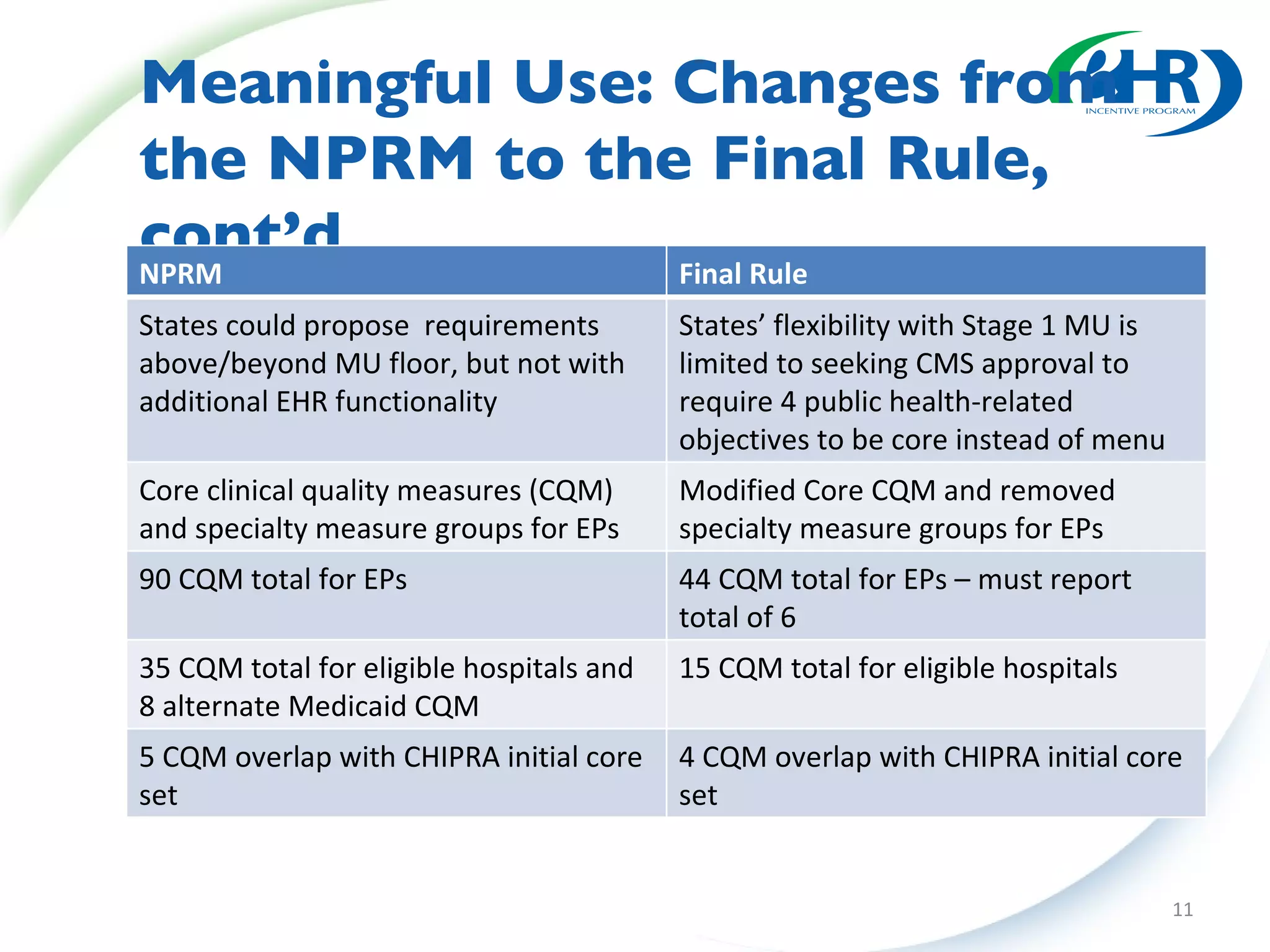
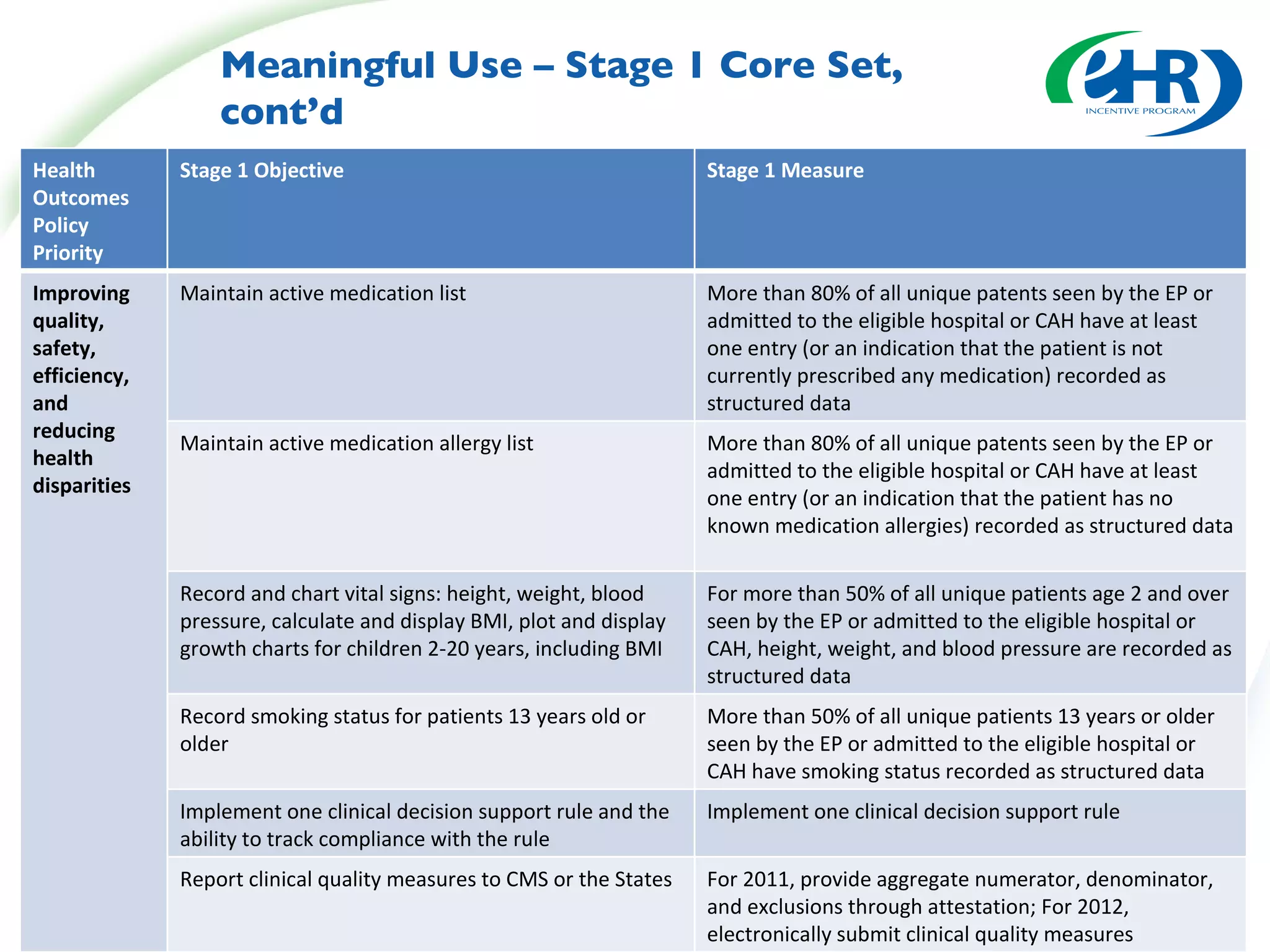
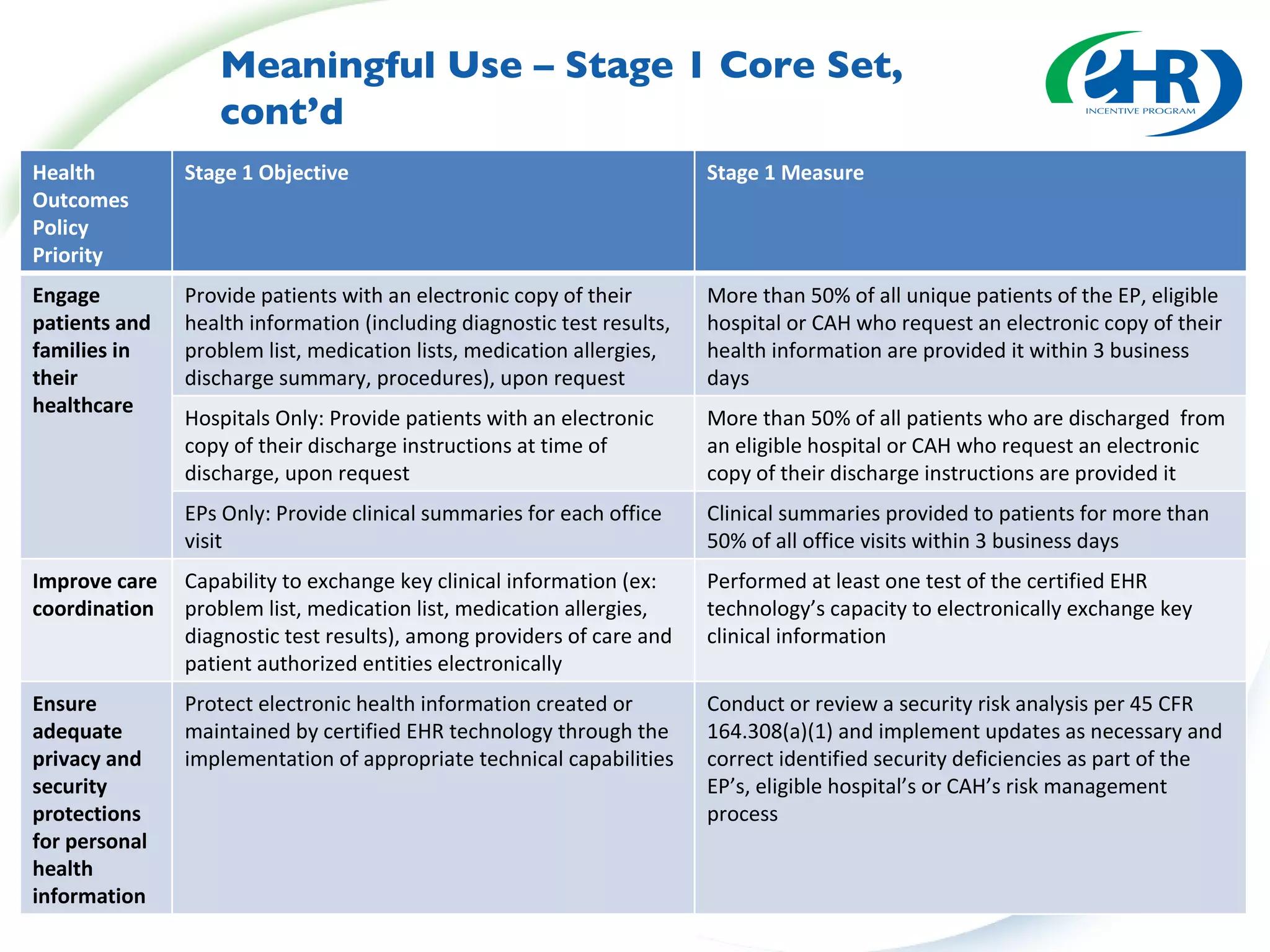
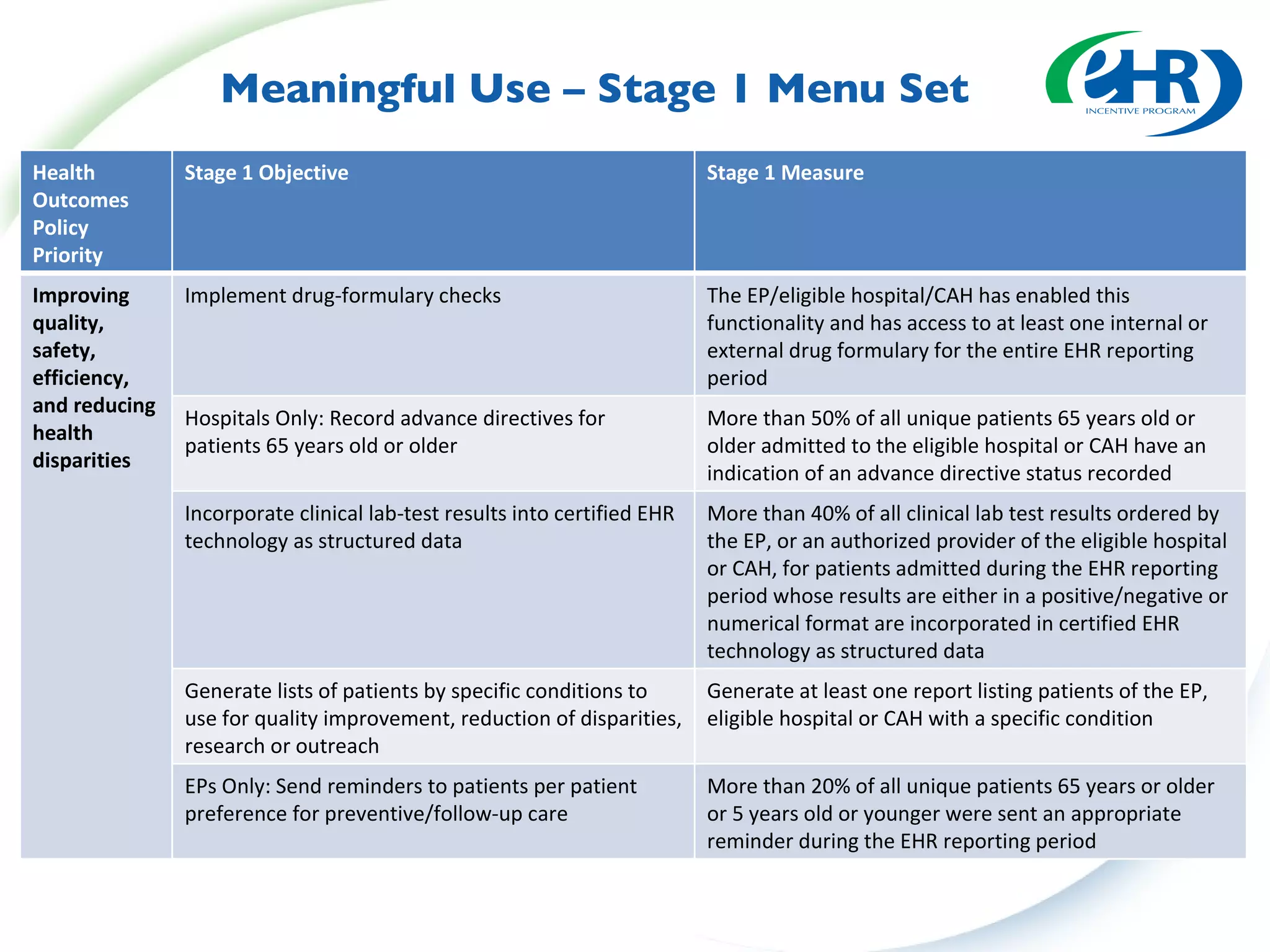
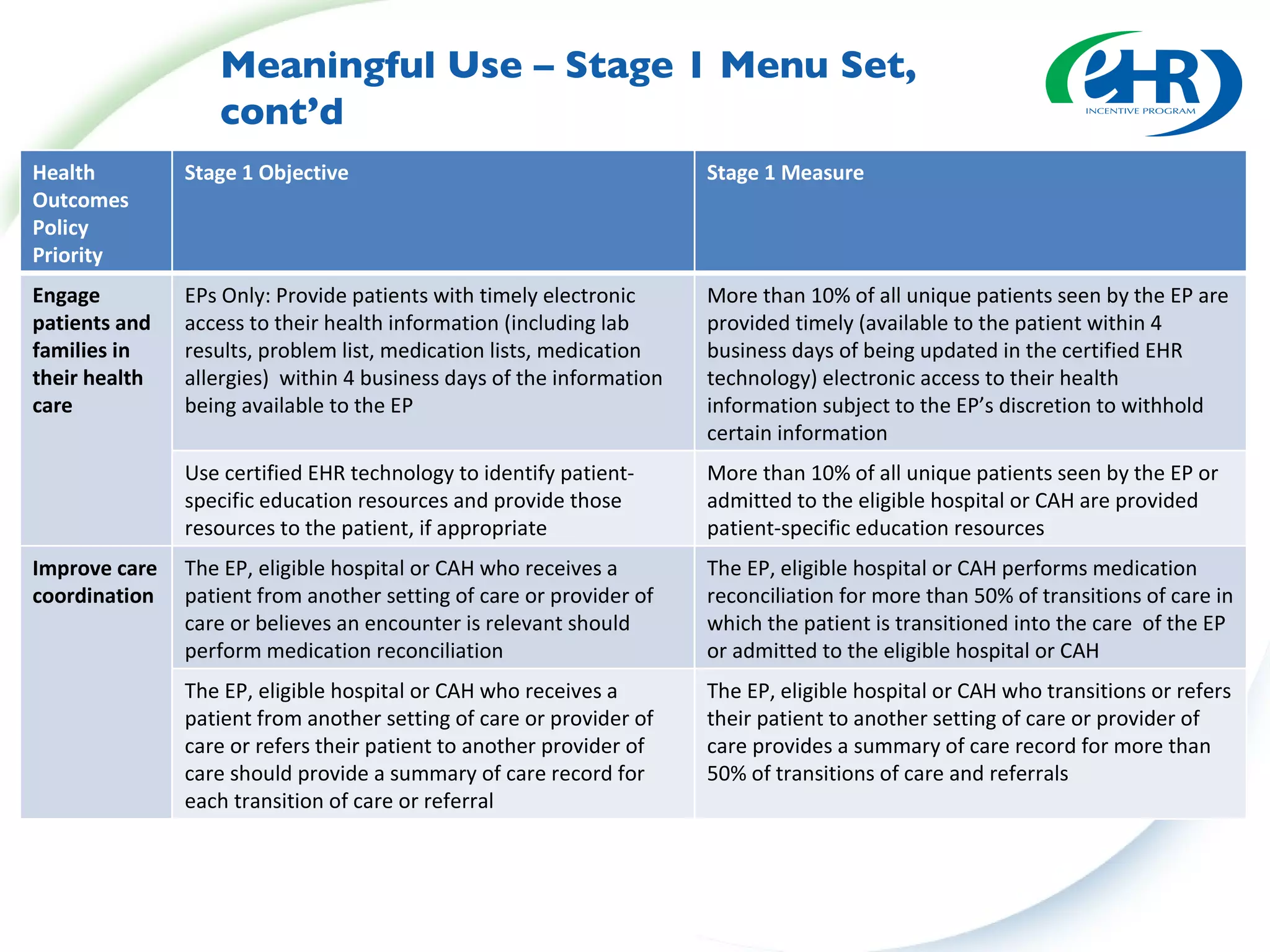
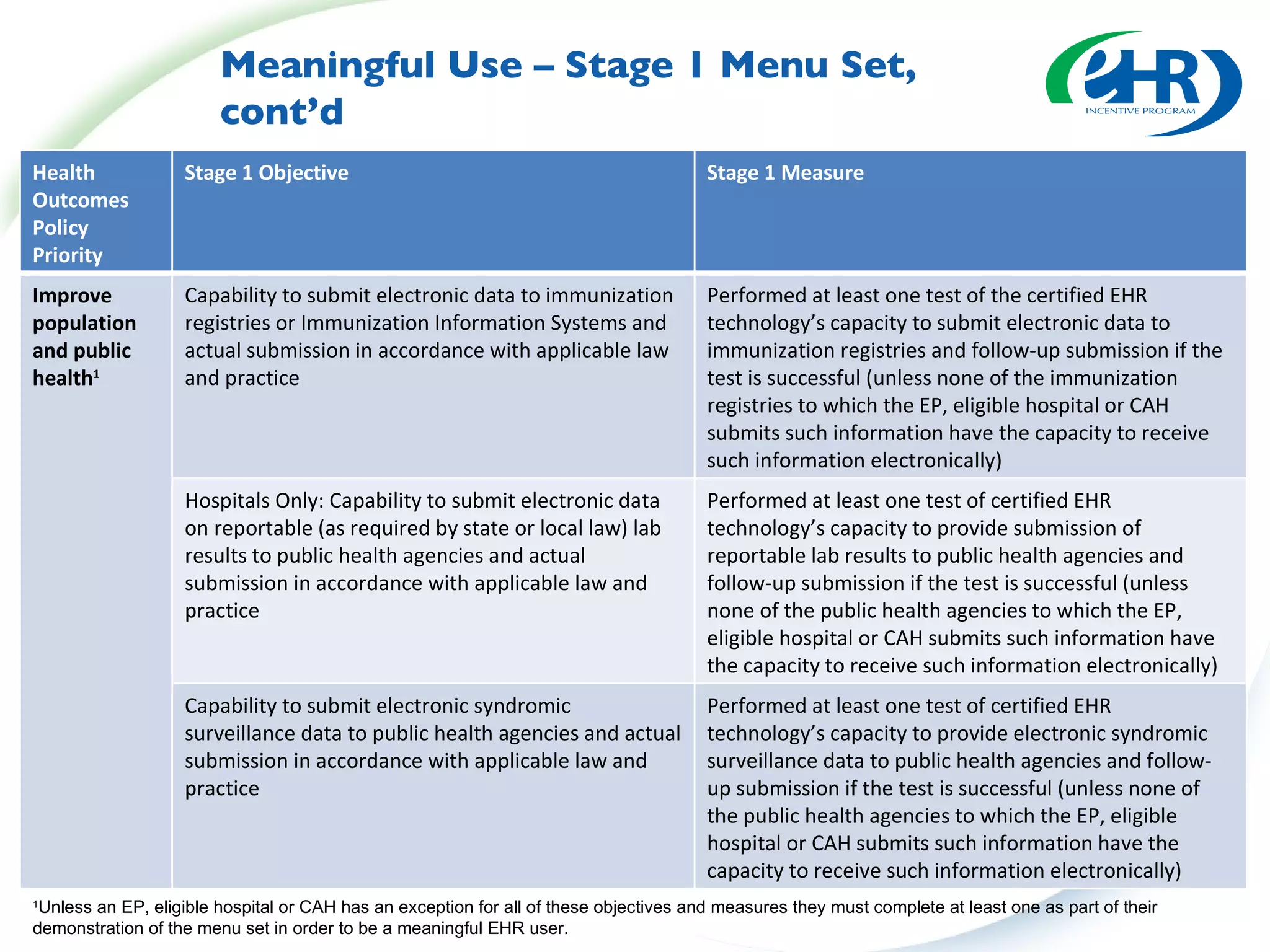
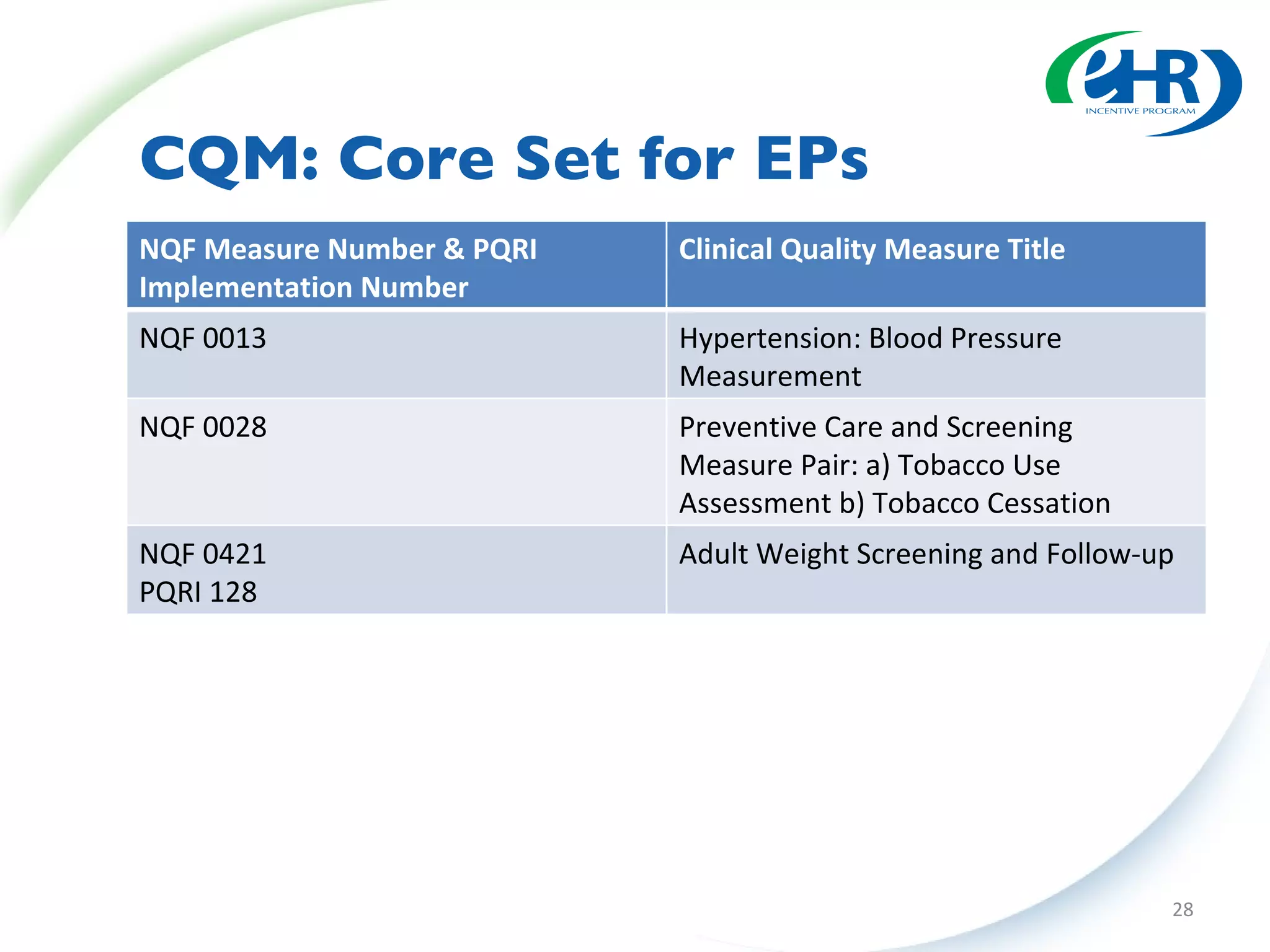
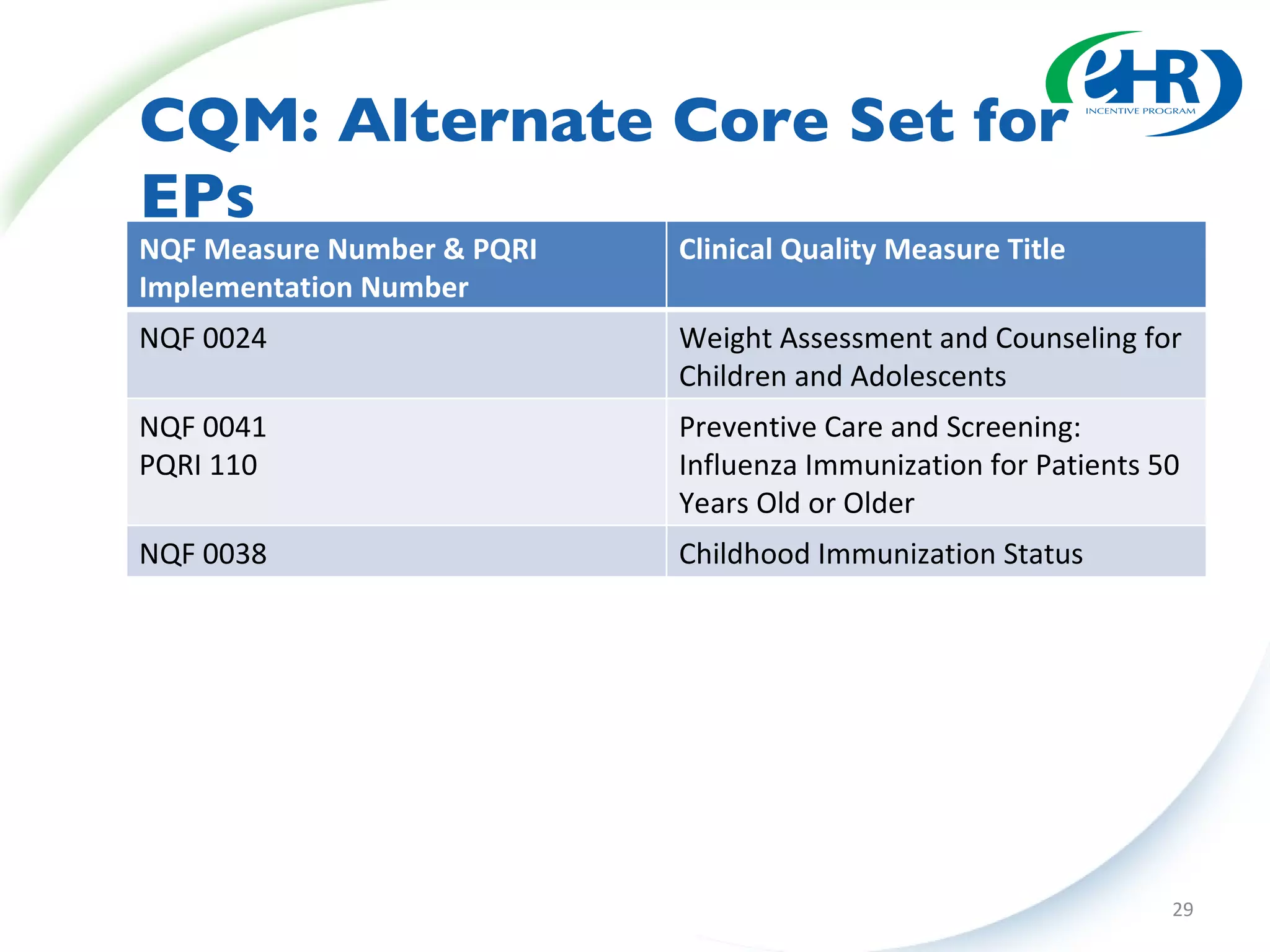
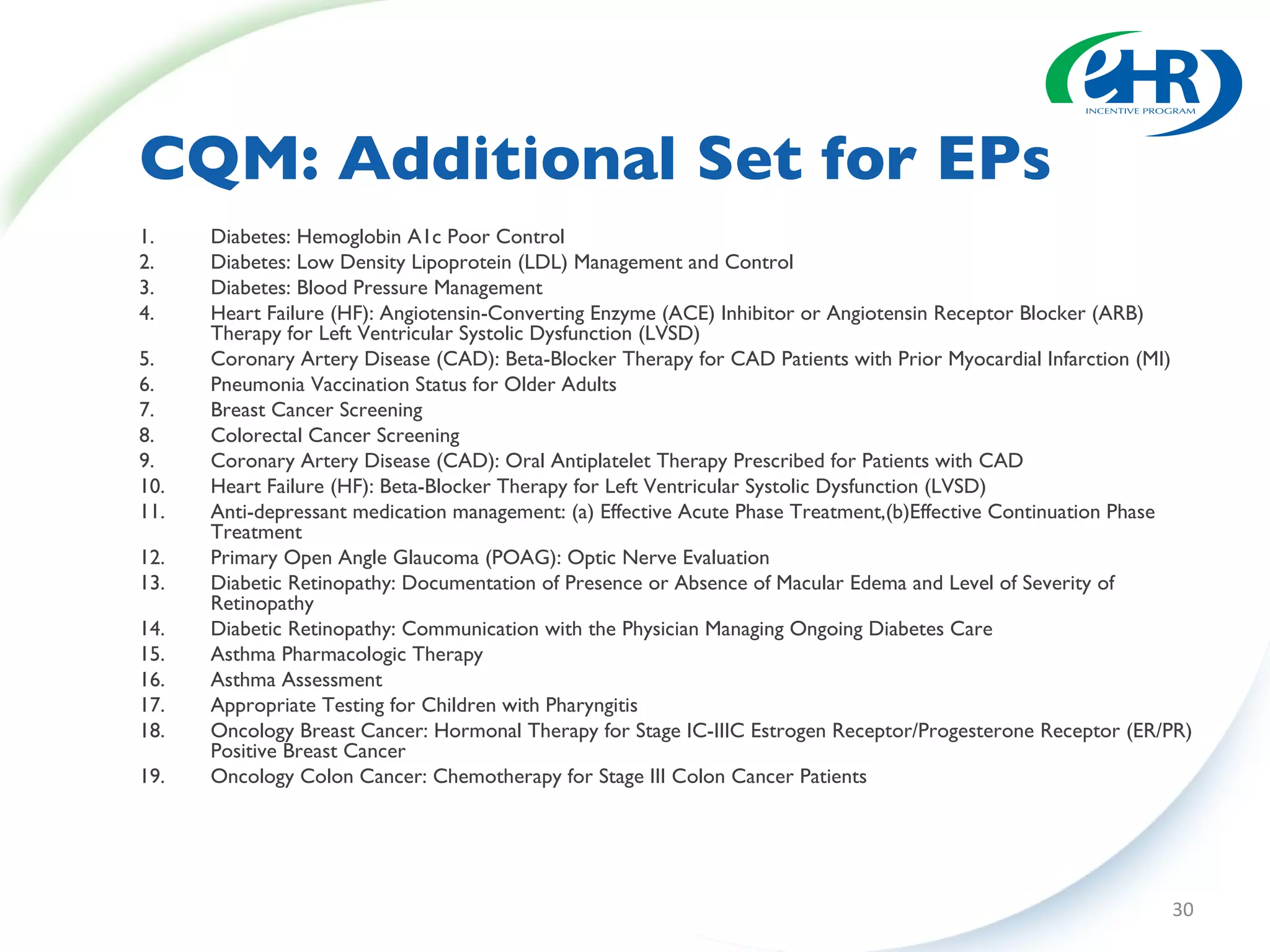
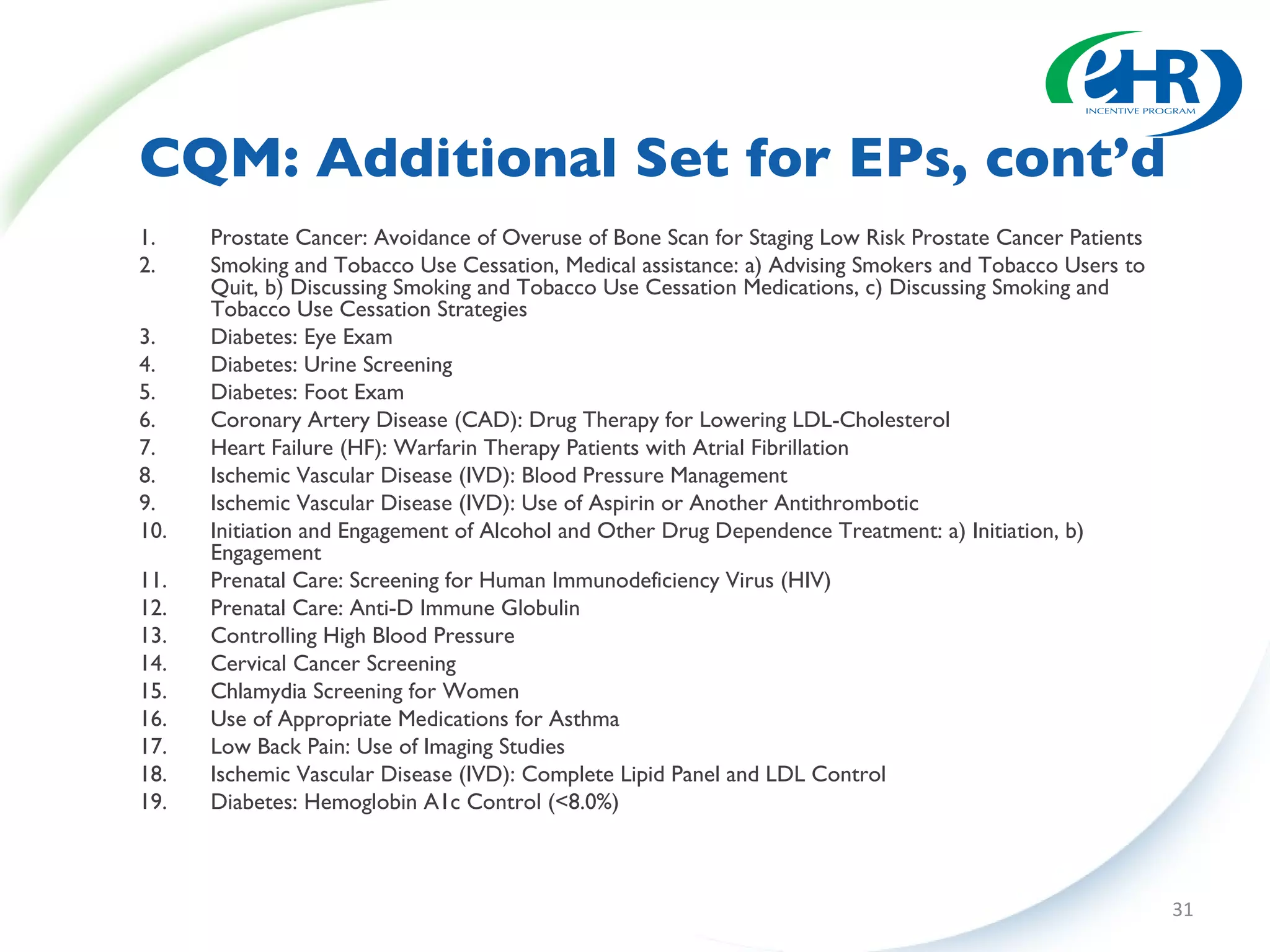
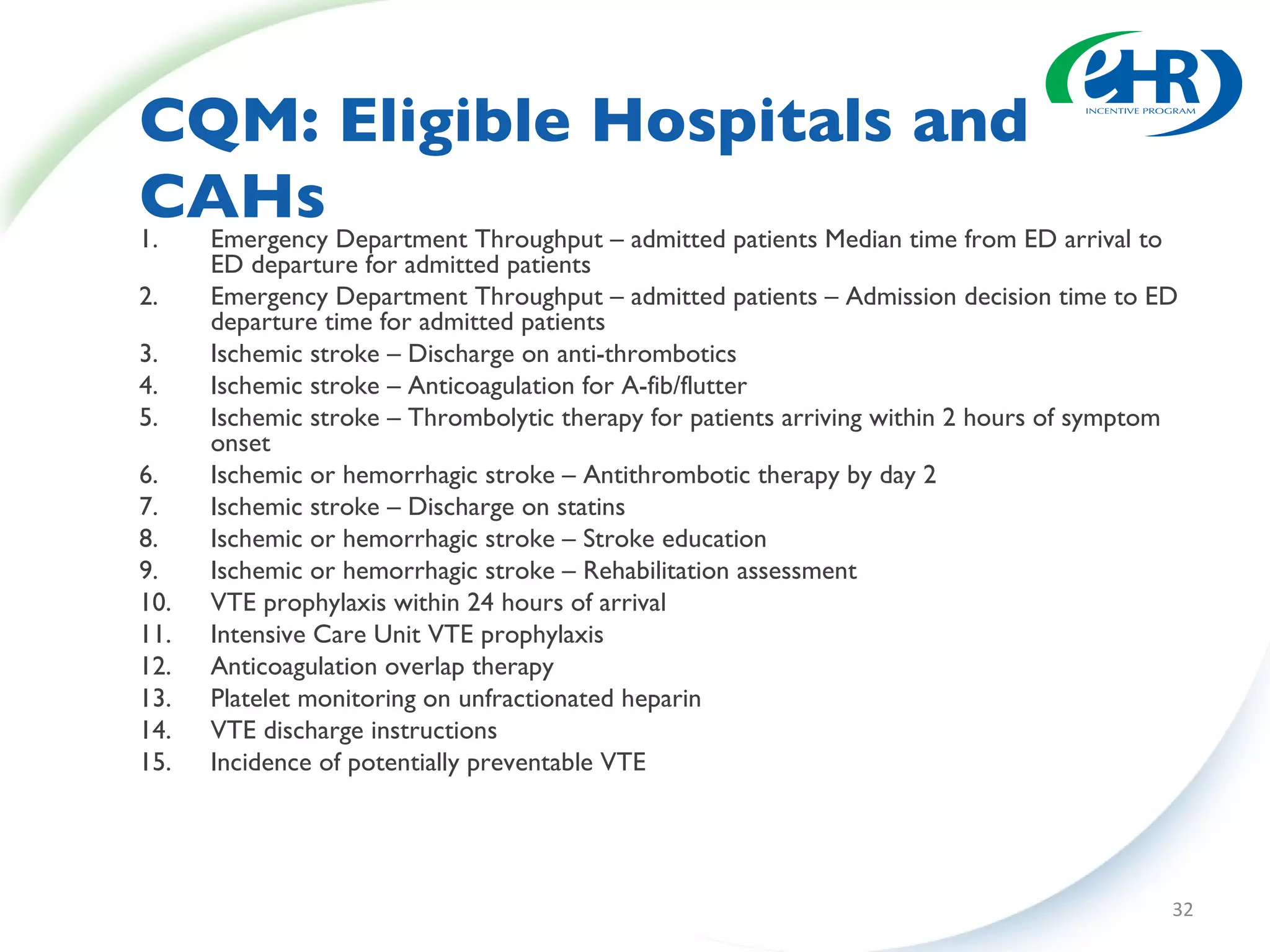
This document summarizes changes from the proposed rule to the final rule for Stage 1 of the Medicare and Medicaid EHR Incentive Program's meaningful use criteria. Key changes included lowering thresholds for some objectives, removing administrative transactions, adding new objectives, and modifying clinical quality measures for eligible professionals. The final rule provided more flexibility for states and clarified various eligibility and reporting requirements.






















![Trudel cms-rules-072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudel-cms-rules-0728101-100810090601-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel Cms Rules 072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudelcmsrules0728101-12814484645456-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

























