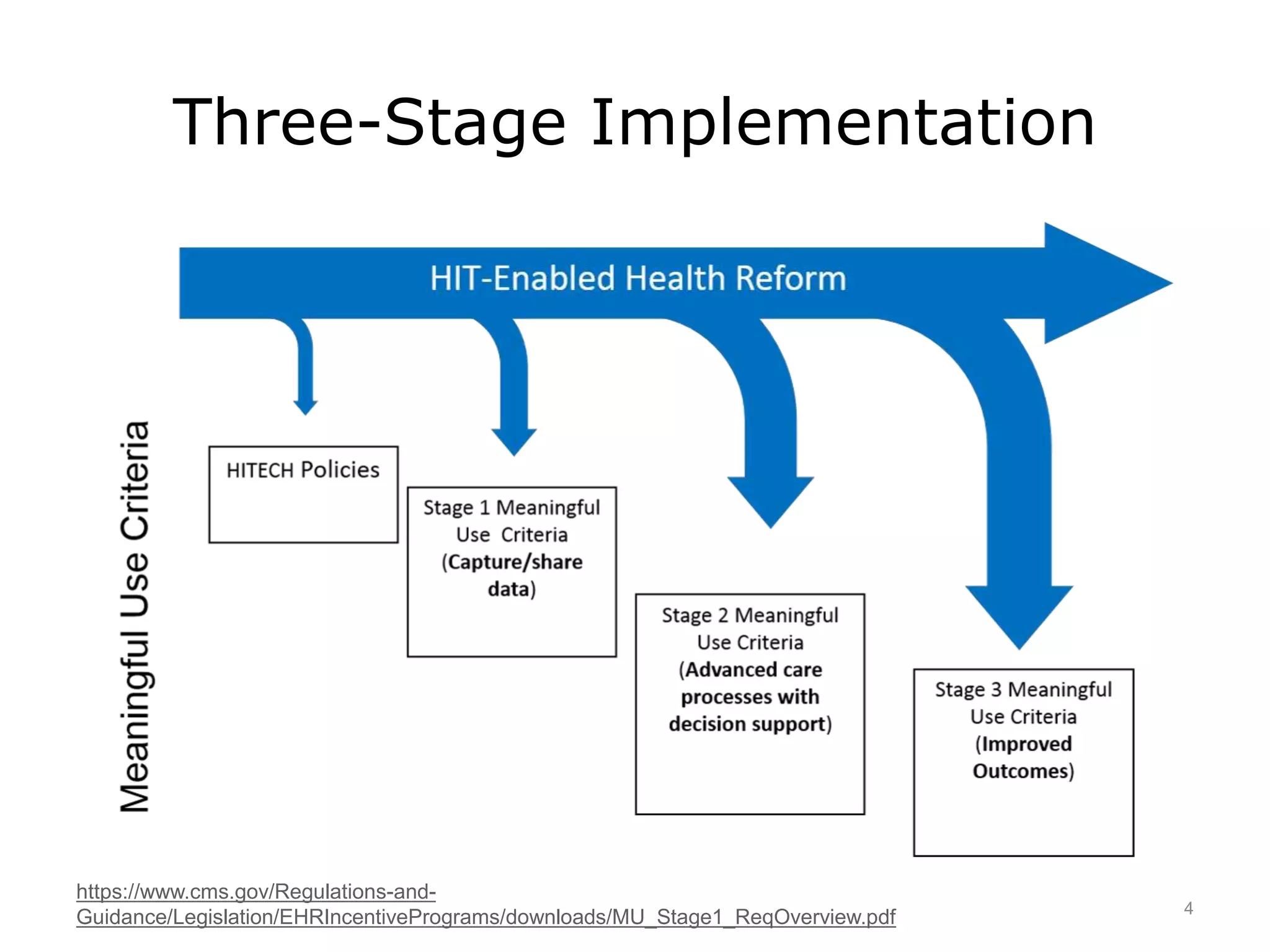
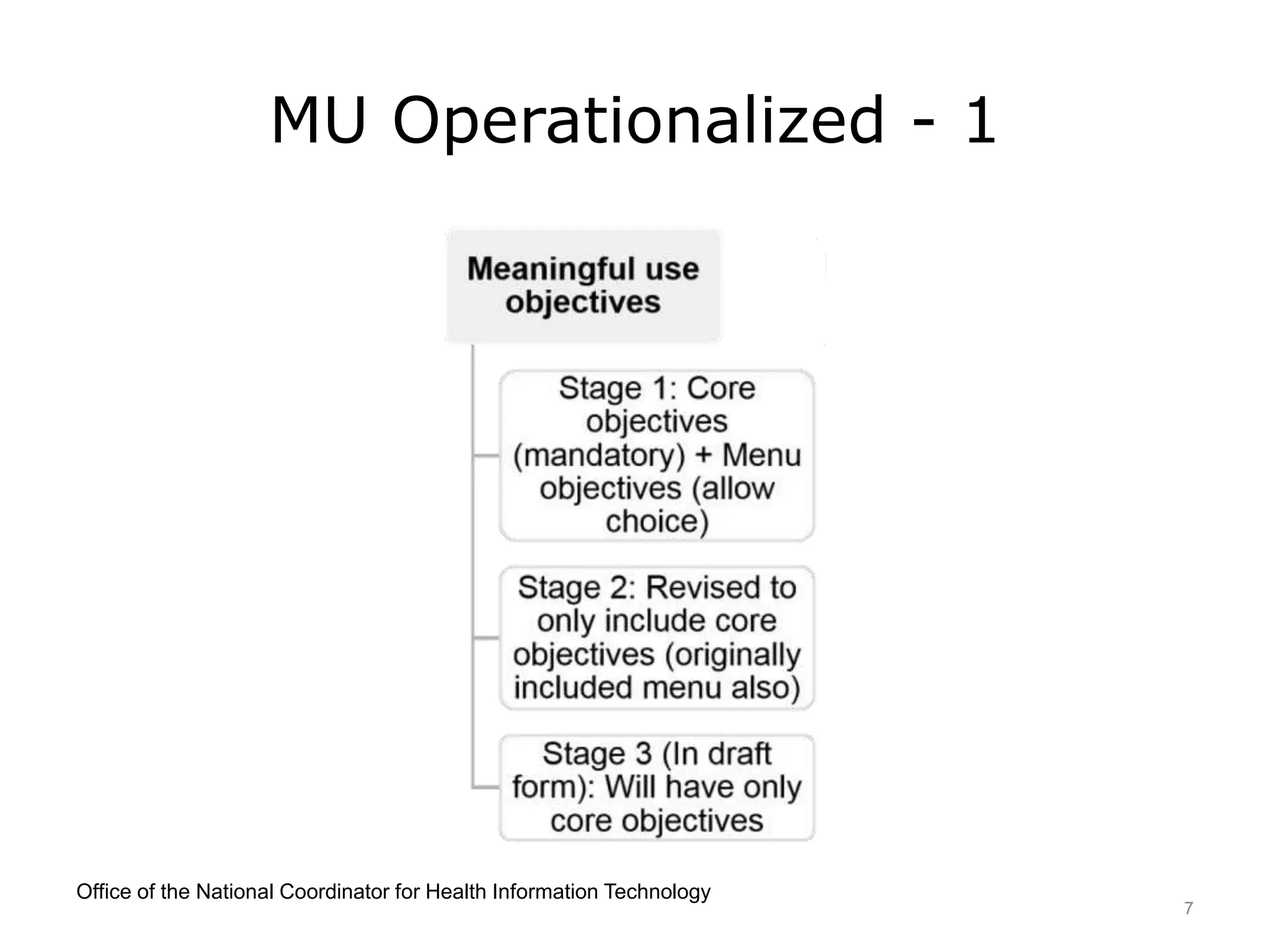
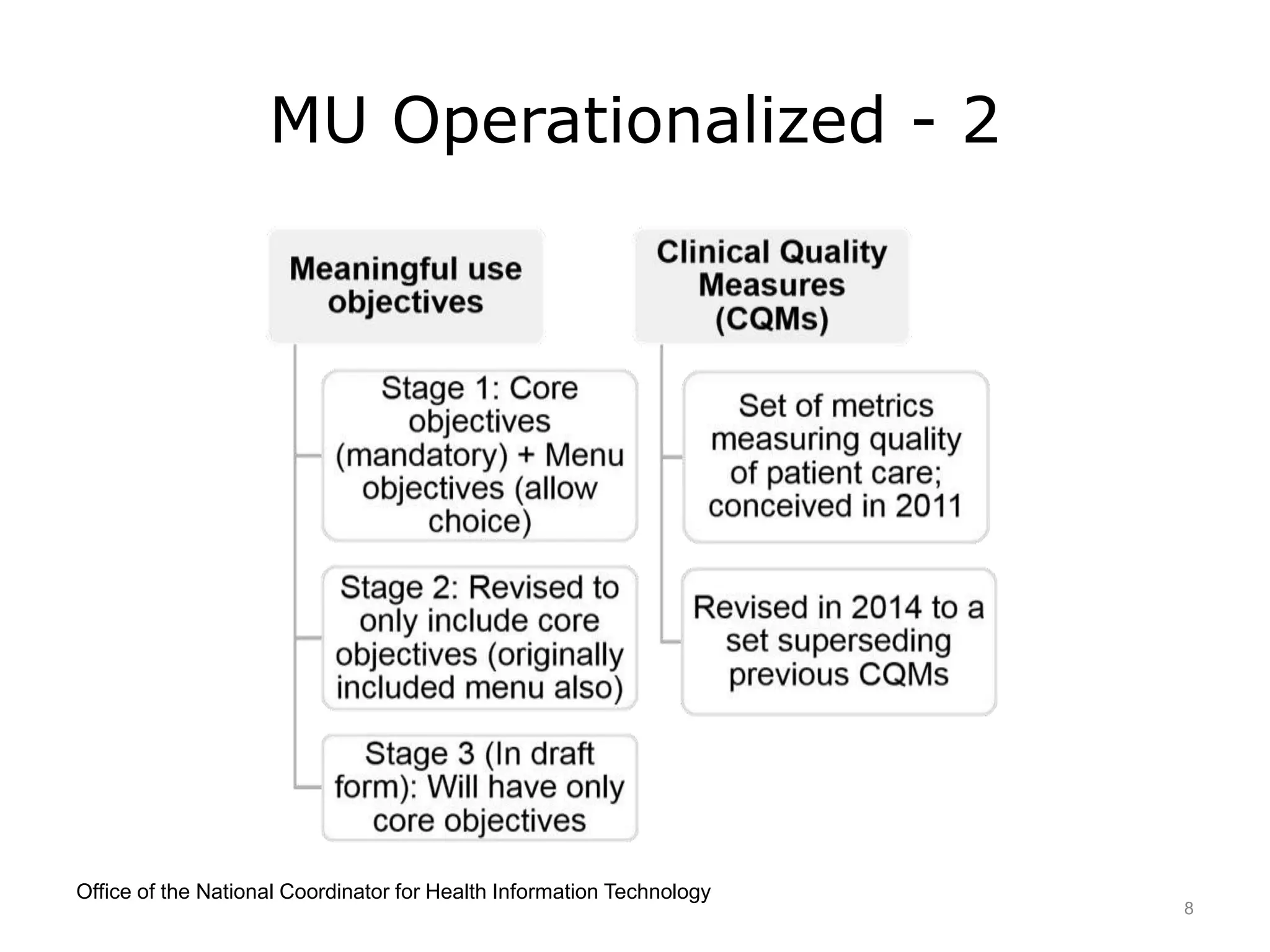
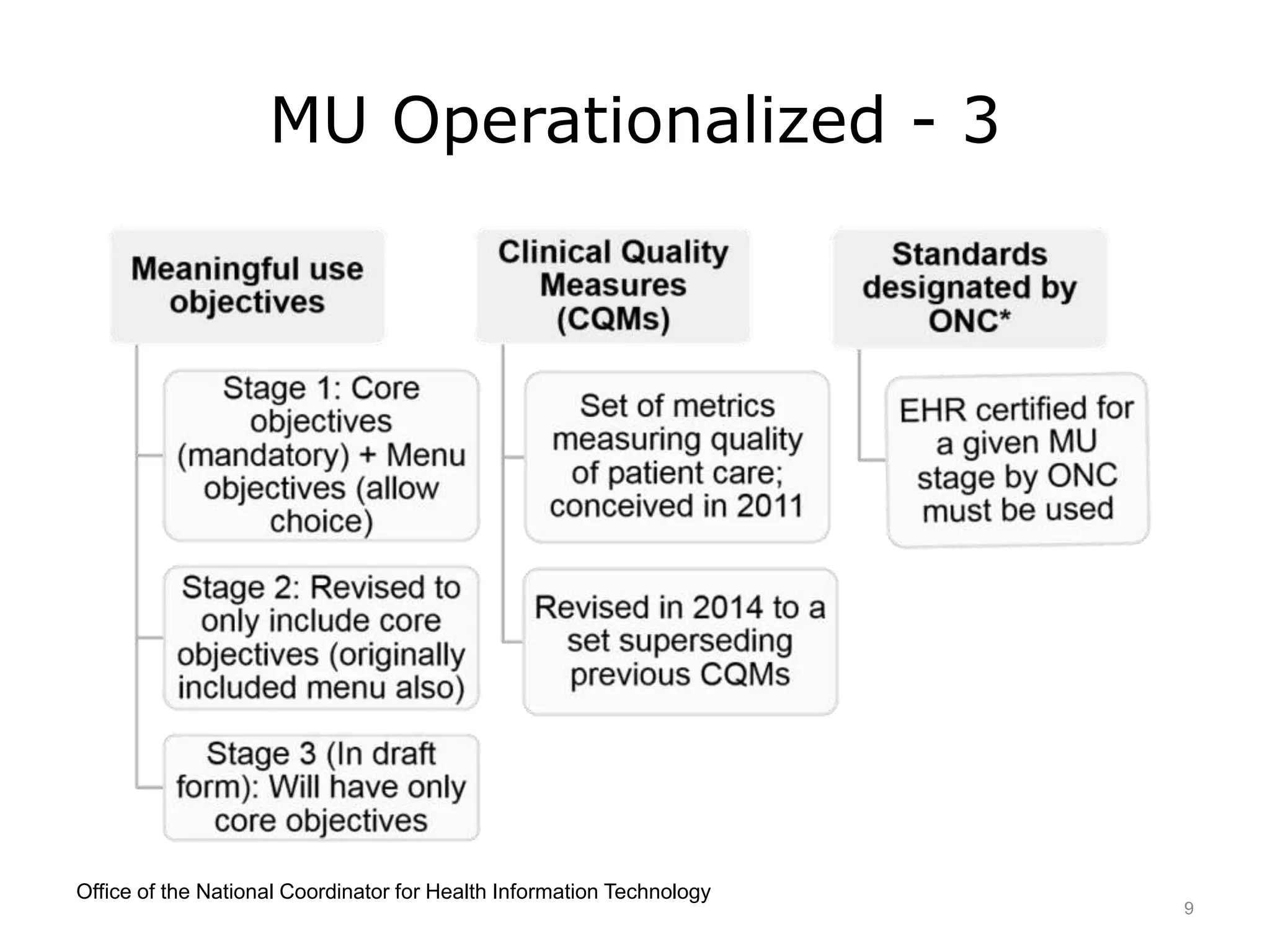
This lecture discusses the implementation of meaningful use (MU) of electronic health records as required by the HITECH Act. It outlines the three stages of MU criteria that eligible professionals and hospitals must meet to receive incentive payments for adopting electronic health records. All providers should now be in Modified Stage 2, which focuses on increased patient engagement, exchange of clinical summaries between providers, and other objectives. The goals of MU and HITECH are to advance the use of health IT and encourage nationwide health information exchange.