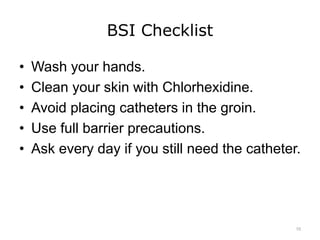
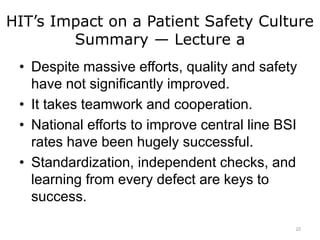
This document is a lecture on how health information technology (HIT) can impact patient safety culture. It discusses applying quality improvement tools to analyze HIT errors. It highlights the success of efforts led by Dr. Peter Pronovost to reduce central line bloodstream infections through standardization, independent checks, and learning from defects. Checklists, data collection, and adopting practices from high-reliability industries like aviation and Toyota have helped significantly reduce infection rates.



![HIT’s Impact on a Patient Safety Culture
References — Lecture a — 1
References
Klein, S., & McCarthy, D. (2010 April/May). A conversation with Peter Pronovost about
patient safety. Quality Matters. Retrieved May 25, 2016, from
http://www.commonwealthfund.org/Newsletters/Quality-Matters/2010/April-May-
2010/Q--A.aspx
Pronovost, P. (2010 October). Speech presented at the Legg Mason Capital
Management Thought Leader Forum.
Ross, B. (2010 January 29). Toyota CEO apologizes to his customers: ‘I am deeply
sorry.’” ABC News. Retrieved May 25, 2016, from
http://abcnews.go.com/Blotter/toyota-ceo-apologizes-deeply/story?id=9700622
Charts, Tables, Figures
7.01 Figure: Key Topics. Courtesy Dr. Anna Maria Izquierdo-Porrera.
Images
Slide 3: Dr. Peter Pronovost Listens to a Patient’s Heart [Online image]. The photo was
taken during filming for Program One — "Silent Killer" at Johns Hopkins
University's Hospital and Children's Center for the RAM Campaign. Retrieved May
25, 2016, from http://www.ramcampaign.org/pages/campaign_photos.htm
23](https://image.slidesharecdn.com/comp12unit7alectureslides-190828200145/85/lecture-7A-23-320.jpg)
![HIT’s Impact on a Patient Safety Culture
References — Lecture a — 2
Images
Slide 4: Dr. Peter Pronovost [Online image]. The photo was taken during filming for
Program One — "Silent Killer" at Johns Hopkins University's Hospital and Children's
Center for the RAM Campaign. Retrieved May 25, 2016, from
http://www.ramcampaign.org/pages/campaign_photos.htm
Slide 6: Earthrise Over the Lunar Horizon [Online image].(NASA photo ID AS11-44-6552).
Retrieved May 25, 2016, from
http://nssdc.gsfc.nasa.gov/planetary/lunar/apollo11.html
Slide 7: Planet Earth from the Moon [Online image]. (NASA photo ID AS11-36-5355).
Retrieved May 25, 2016, from
http://nssdc.gsfc.nasa.gov/planetary/lunar/apollo11.html
Slide 8: A Collage of Association Logos for Agencies Involved in HIT. Image Sources,
retrieved March 2012: Agency for Healthcare Research and Quality.
http://www.ahrq.gov/; VA National Center for Patient Safety.
http://www.patientsafety.va.gov/ World Health Organization. www.who.int; Joint
Commission. http://www.jointcommission.org/; American Medical Association.
http://www.ama-assn.org/; Institute for Safe Medication Practices.
http://www.ismp.org; Consumers Advancing Patient Safety.
http://www.patientsafety.org; ECRI Institute. https://www.ecri.org; National Patient
Safety Foundation. http://www.npsf.org; National Center for Nursing Quality.
http://www.nursingworld.org/ncnq
24](https://image.slidesharecdn.com/comp12unit7alectureslides-190828200145/85/lecture-7A-24-320.jpg)
![HIT’s Impact on a Patient Safety Culture
References — Lecture a — 3
Images
Slide 9: 2009 National Healthcare Disparities Reports and National Healthcare Quality
Report. Agency for Healthcare Research and Quality, Rockville, MD. Retrieved May
27, 2016 from: http://archive.ahrq.gov/research/findings/nhqrdr/nhdr09/index.html and
http://archive.ahrq.gov/research/findings/nhqrdr/nhqr09/index.html
Slide 11: A Clinician Prepares a Syringe While a Patient Looks On. American Health
Information Management Association (AHIMA).
Slide 12: A Three-Point Seat Belt in a Lincoln Town Car [Online image]. Creative
Commons: Gerdbrendel. Retrieved May 25, 2016, from
http://en.wikipedia.org/wiki/File:Seatbelt.jpg
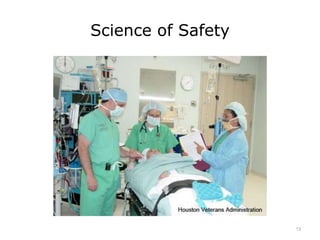
Slide 13: David H. Berger, M.D., MEDVAMC Operative Care Line Executive (Left)
Prepares for Surgery with an Anesthesia Resident and Grace Campos, R. N.,
Operating Room Nurse.
Slide 14: Nurse [Online image]. Educational Resources — National Organization on Fetal
Alcohol Syndrome (NOFAS). Centers for Disease Control. Retrieved May 25, 2016,
from http://www.cdc.gov/ncbddd/fasd/training.html
25](https://image.slidesharecdn.com/comp12unit7alectureslides-190828200145/85/lecture-7A-25-320.jpg)
![HIT’s Impact on a Patient Safety Culture
References — Lecture a — 4
Images
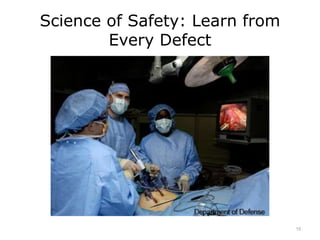
Slide 15: Doctors Ronald Post (Left) and John Smear (Center) and Physician’s Assistant
Debra Blackshire Perform Laparoscopic Stomach Surgery [Online image]. Department of
Defense. Retrieved May 25, 2016, from http://www.defense.gov/Media/Photo-
Gallery?igphoto=2001242690
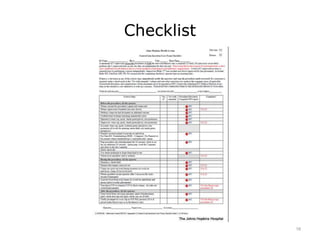
Slide 16: Blood Infection Checklist at Johns Hopkins. Available
from:http://www.hopkinsmedicine.org
Slide 17: Swan-Ganz-Heparin Coated Catheter. FDA.
https://www.fda.gov/MedicalDevices/default.htm
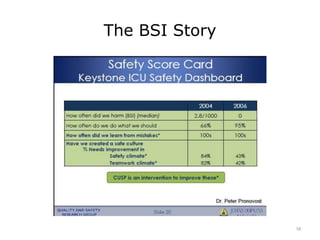
Slide 18: Safety Score Card. The BSI Report Card – Dr. Peter Pronovost. Johns Hopkins
Hospital.
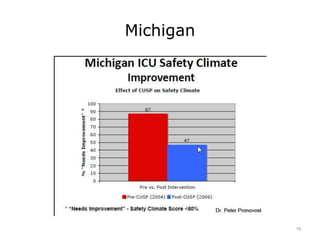
Slide 19: Overview of STOP-BSI Program. Peter Pronovost, MD, PhD. Johns Hopkins
Hospital.
Slide 20: The Model. Johns Hopkins Hospital. http://www.hopkinsmedicine.org
Slide 21: Dr. Peter Pronovost [Online image]. Retrieved May 25, 2016, from
http://www.ramcampaign.org/pages/images/Dr_Pronovost_large.jpg
26](https://image.slidesharecdn.com/comp12unit7alectureslides-190828200145/85/lecture-7A-26-320.jpg)