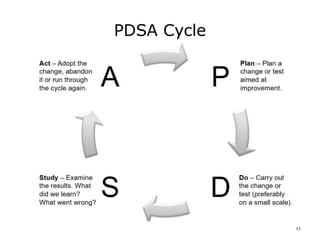
This document provides an overview of quality improvement methods for healthcare settings. It describes strategies for quality improvement, including the role of leadership in creating a culture that supports quality improvement. The document discusses concepts like the PDSA cycle and foundations of quality improvement developed by thinkers like Shewhart, Deming, and Juran. The goal is to introduce methods that can be used to identify and redesign processes, collect and analyze data, and make improvements to eliminate problems and strategically change healthcare systems over time.
![Quality Improvement Methods
References – Lecture a
References
Califf, R. M. (2006). Translating Clinical Trials into Practice (keynote). Tex Heart Inst J., 33(2), 192-196.
Chang, R. Y. (1999). Continuous Process Improvement (Rev ed.). San Francisco, CA: Jossey-Bass
Pfeiffer.
Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (Eds.). (2000). Institute Of Medicine: To Err is Human:
Building a Safer Health System. Washington, DC: National Academy Press.
Ransom, S. B., Joshi, M. S., & Nash, D. (Eds.). (2004). The Healthcare Quality Book: Vision, Strategy,
and Tools (1 ed.). Chicago, IL: Health Administration Press.
Tague, N.R, (2004) The Quality Toolbox, Second Edition, ASQ Quality Press, 390-392.
Images
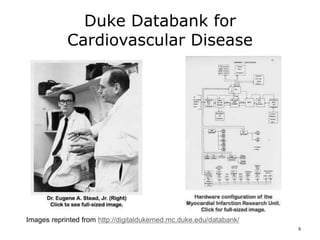
Slide 5: Dr. Eugene A Stead, Jr. [photo]. Retrieved from:
http://digitaldukemed.mc.duke.edu/databank/Images/stead_eugene_thumbnail.jpg
Slide 5: Hardware Configuration [image]. Retrieved from:
http://digitaldukemed.mc.duke.edu/databank/Images/hardware_configuration_1971.jpg
13](https://image.slidesharecdn.com/comp12unit6alectureslides-190828195539/85/Lecture-6A-13-320.jpg)


























![[287 met]](https://cdn.slidesharecdn.com/ss_thumbnails/287met-110424045922-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)