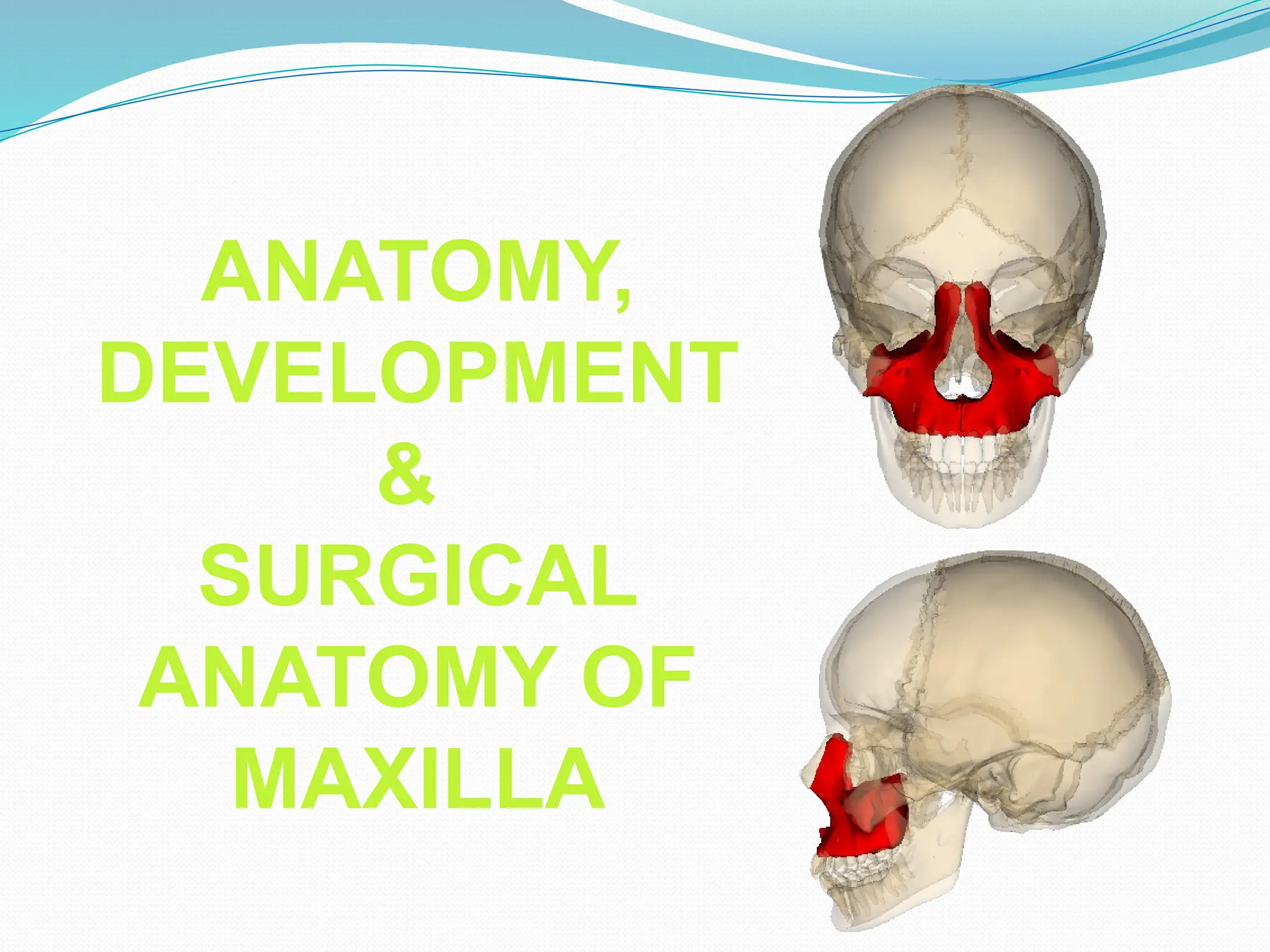
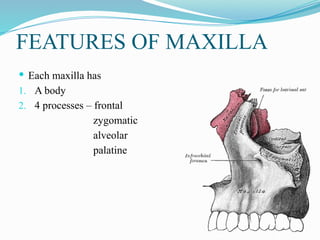
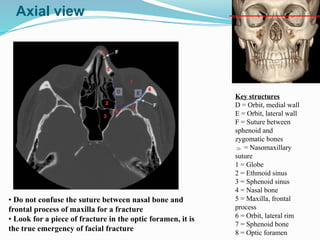
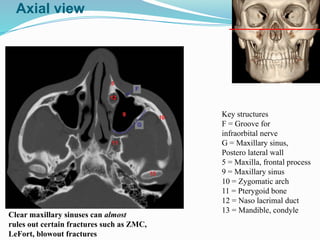
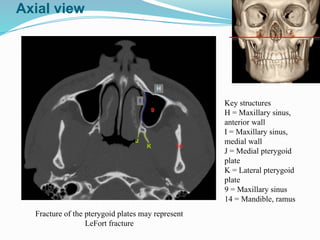
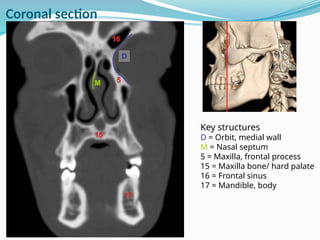
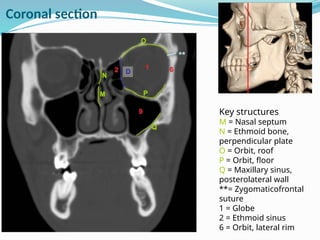
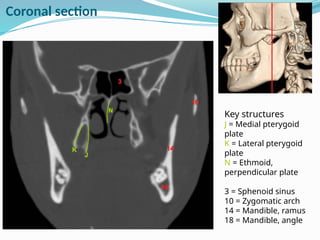
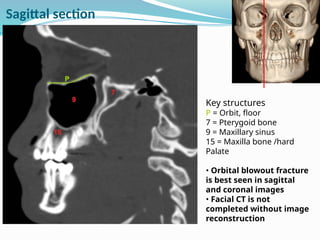
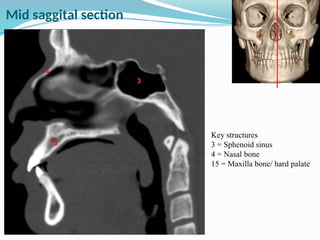
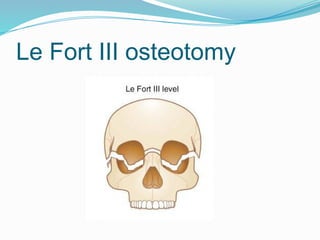
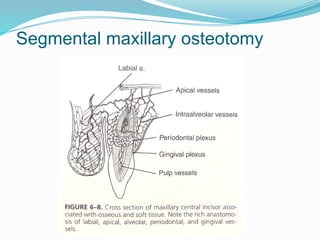
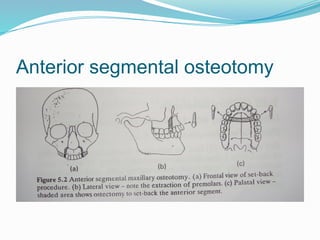
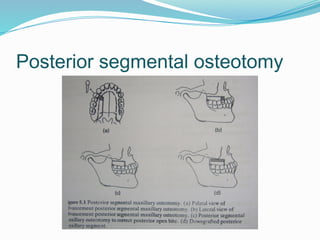
The document provides a detailed overview of the anatomy, development, and surgical aspects of the maxilla, including its formation, features, and articulations with other facial bones. It also describes age-related changes in the maxilla and classifies various types of maxillary fractures, such as Le Fort fractures, with emphasis on typical imaging findings and clinical implications. Surgical anatomy is highlighted, noting the significance of imaging techniques for diagnosing fractures and understanding maxillary structures.