Downloaded 495 times


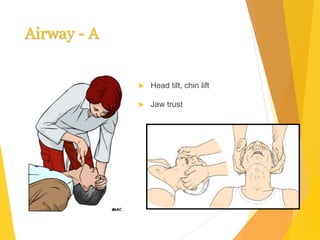
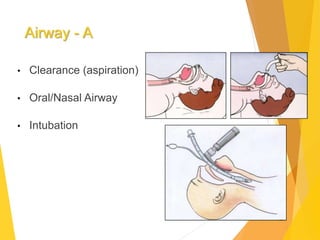
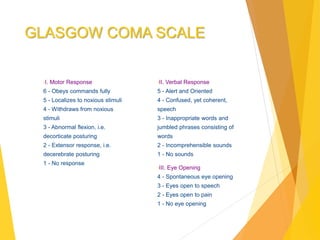







The document provides an overview of the management of unconscious patients, detailing the definition, common causes, diagnosis, and treatment approaches. It outlines the importance of assessing airway, breathing, circulation, disability, and exposure (ABCDE) in unconscious cases, as well as the Glasgow Coma Scale for evaluating consciousness levels. Additionally, it covers the need for a thorough history, physical examination, laboratory tests, and imaging to determine the underlying causes and appropriate medical interventions.

































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

