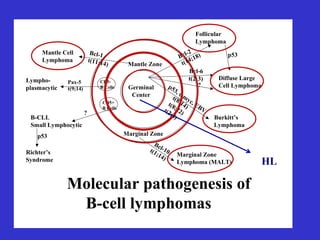
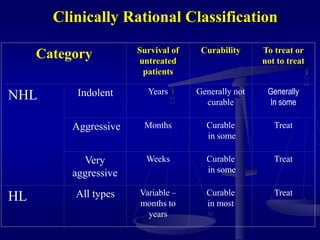
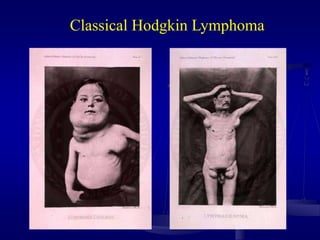
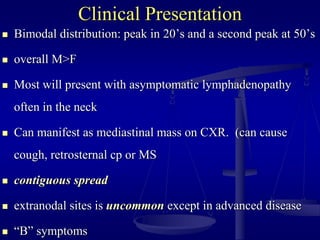
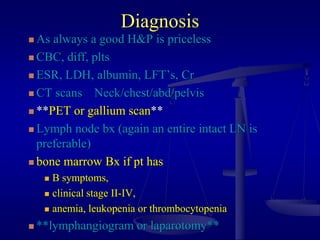
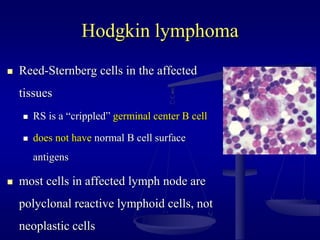
This document discusses lymphomas, including malignant lymphoma concepts, classification, epidemiology, and approaches to lymphoma patients. It focuses on Hodgkin's lymphoma, covering the clinical presentation, diagnosis, histologic subtypes, associated factors, treatment approaches, chemotherapy regimens, prognostic factors, and treatment recommendations for early and advanced stage Hodgkin's lymphoma.



















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















