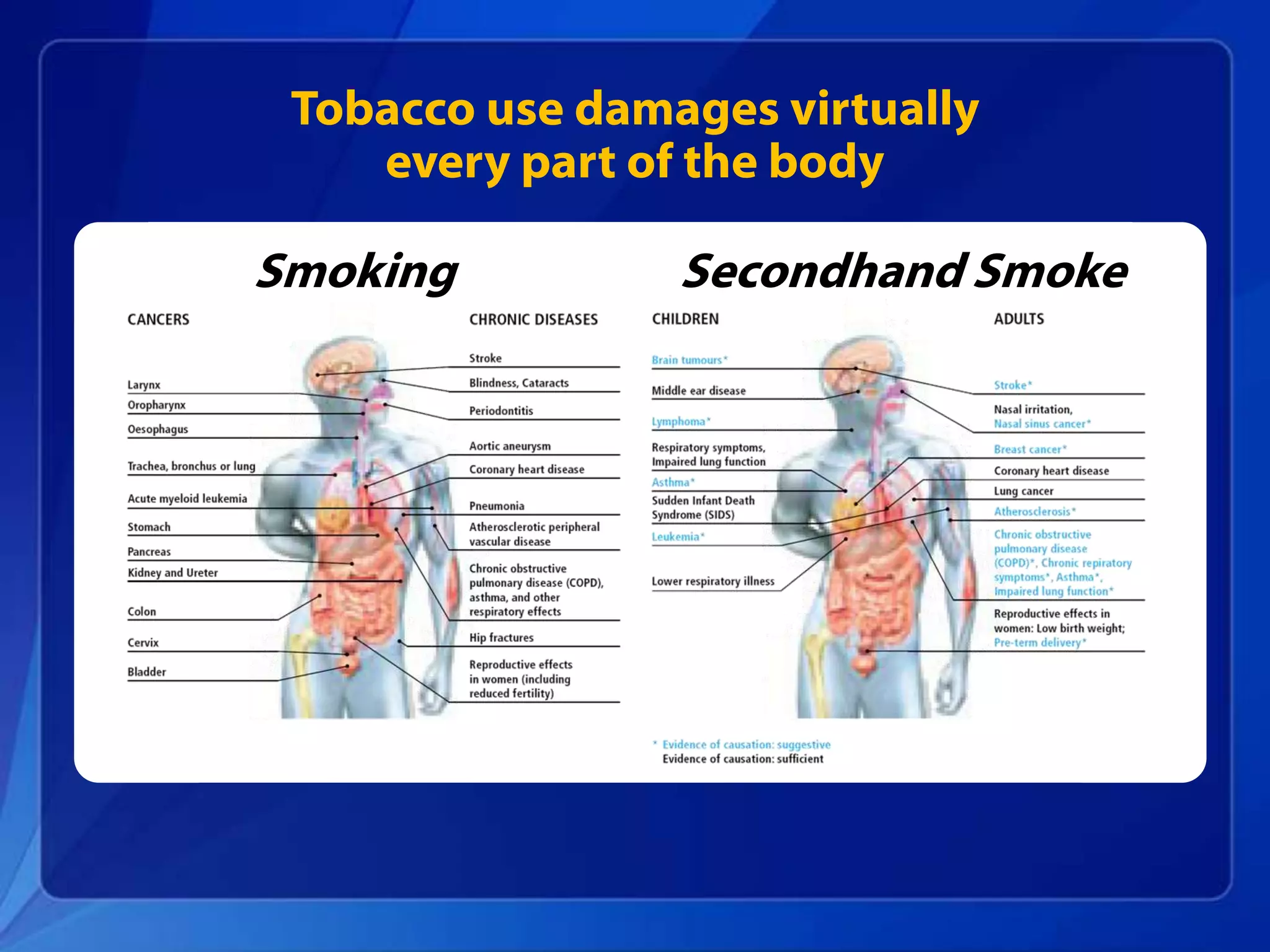
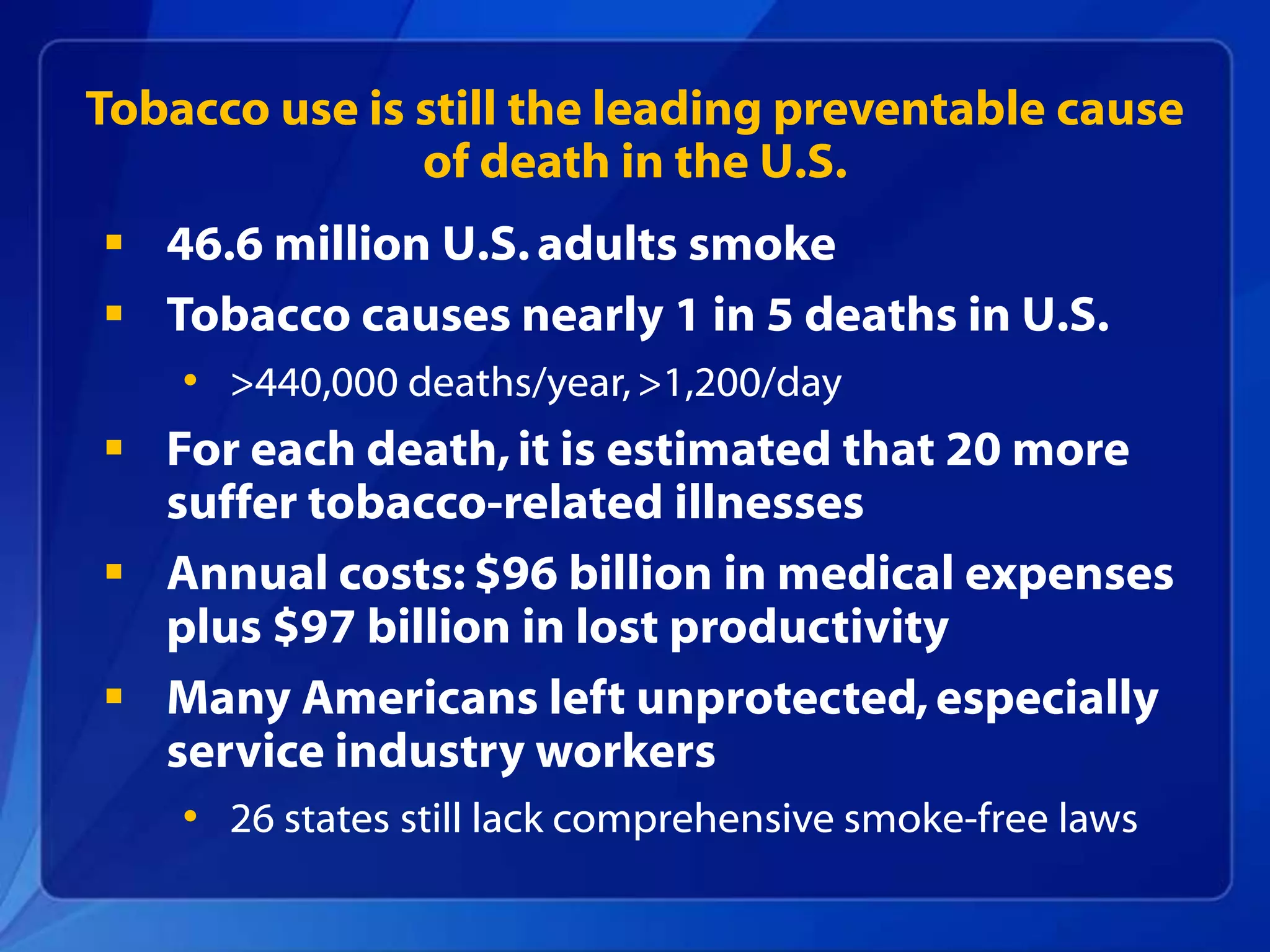
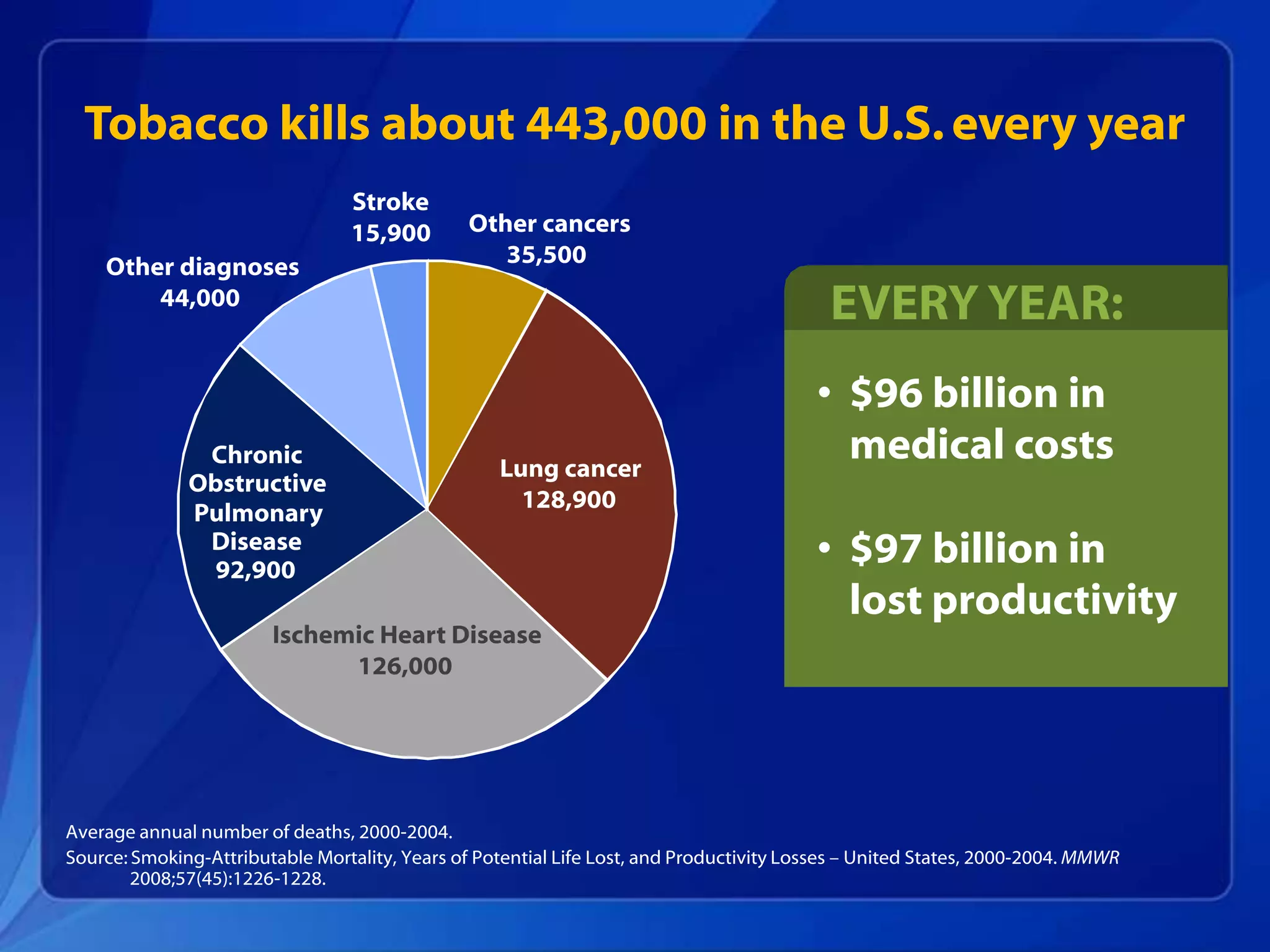
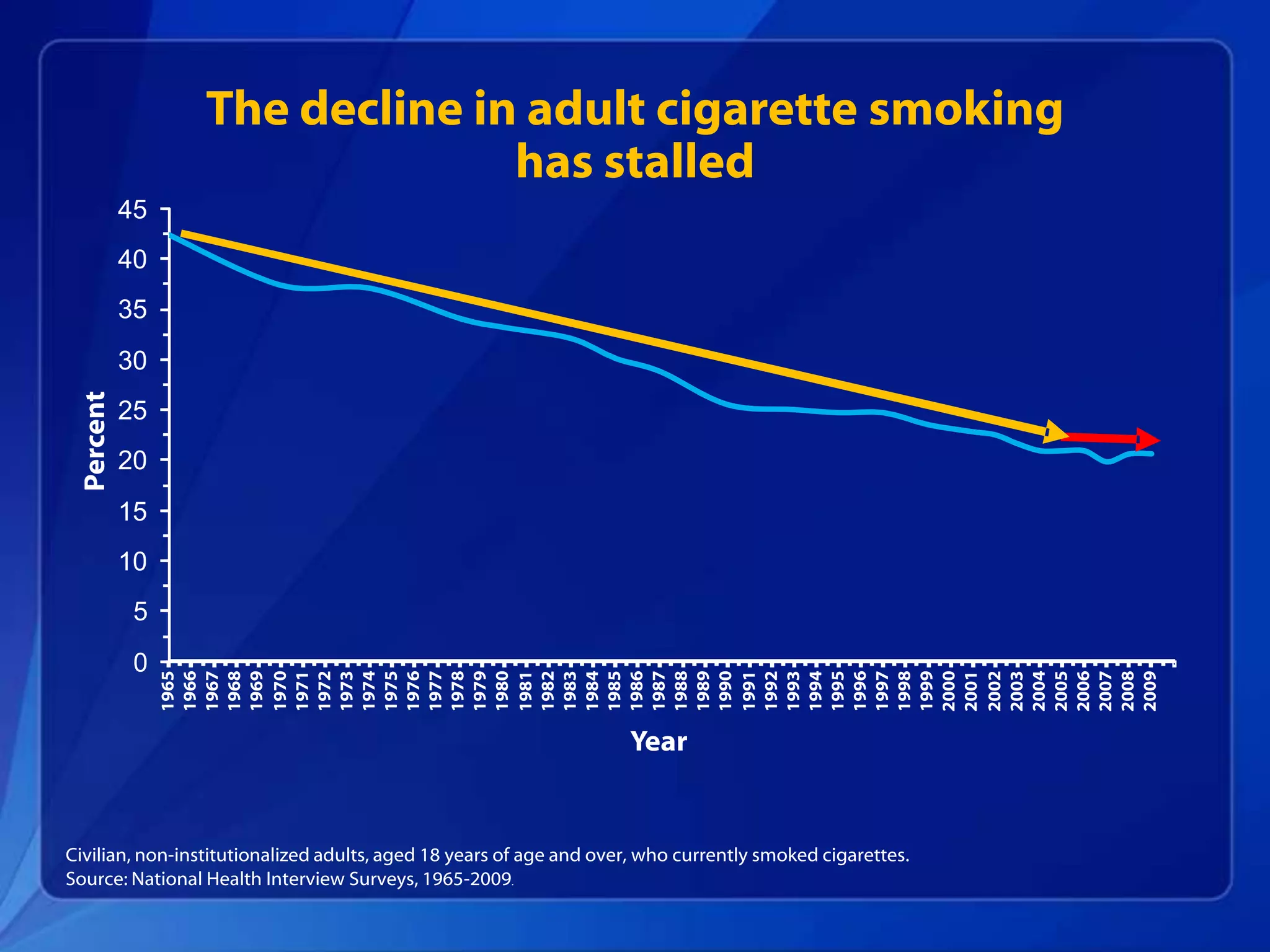
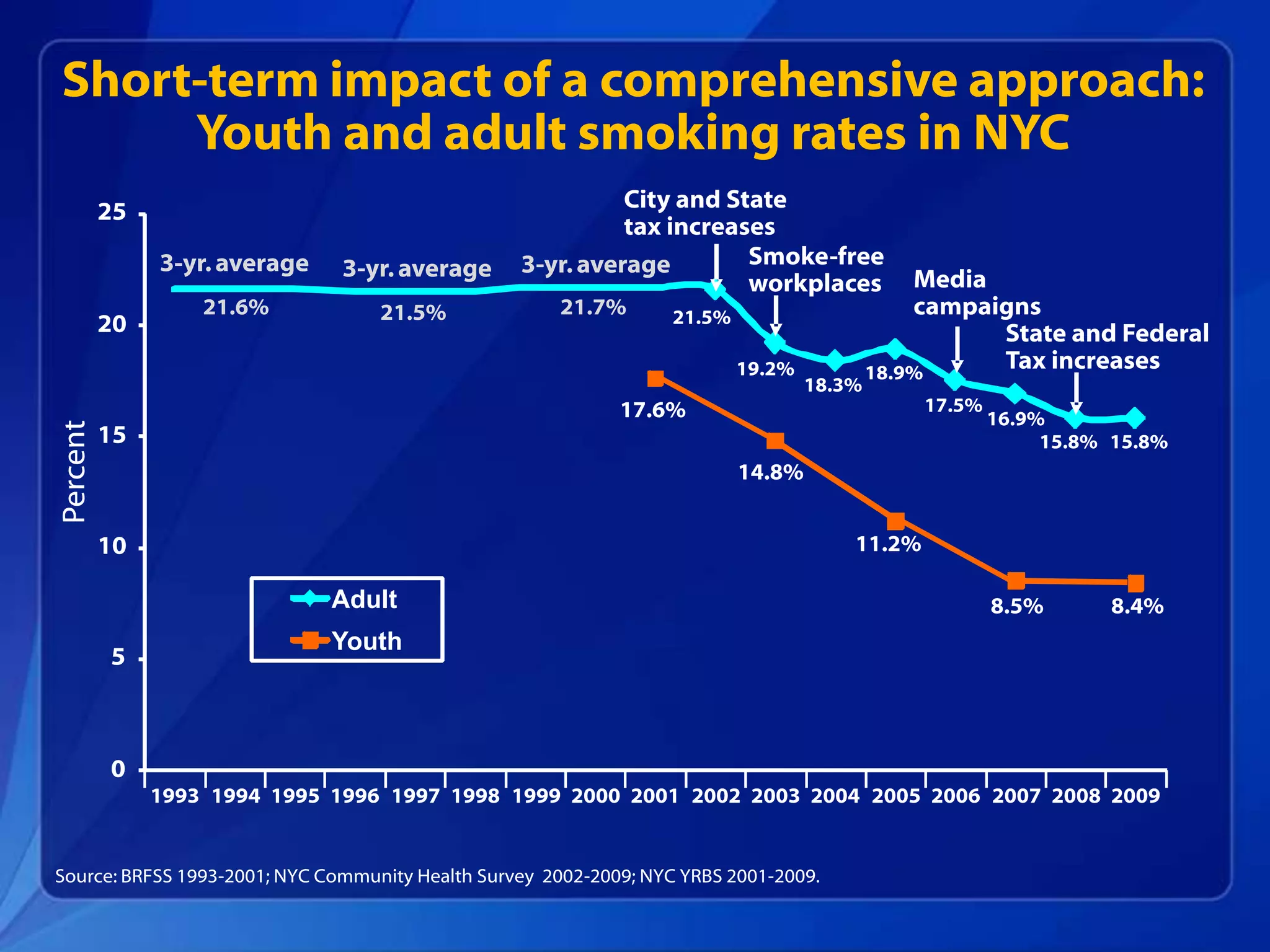
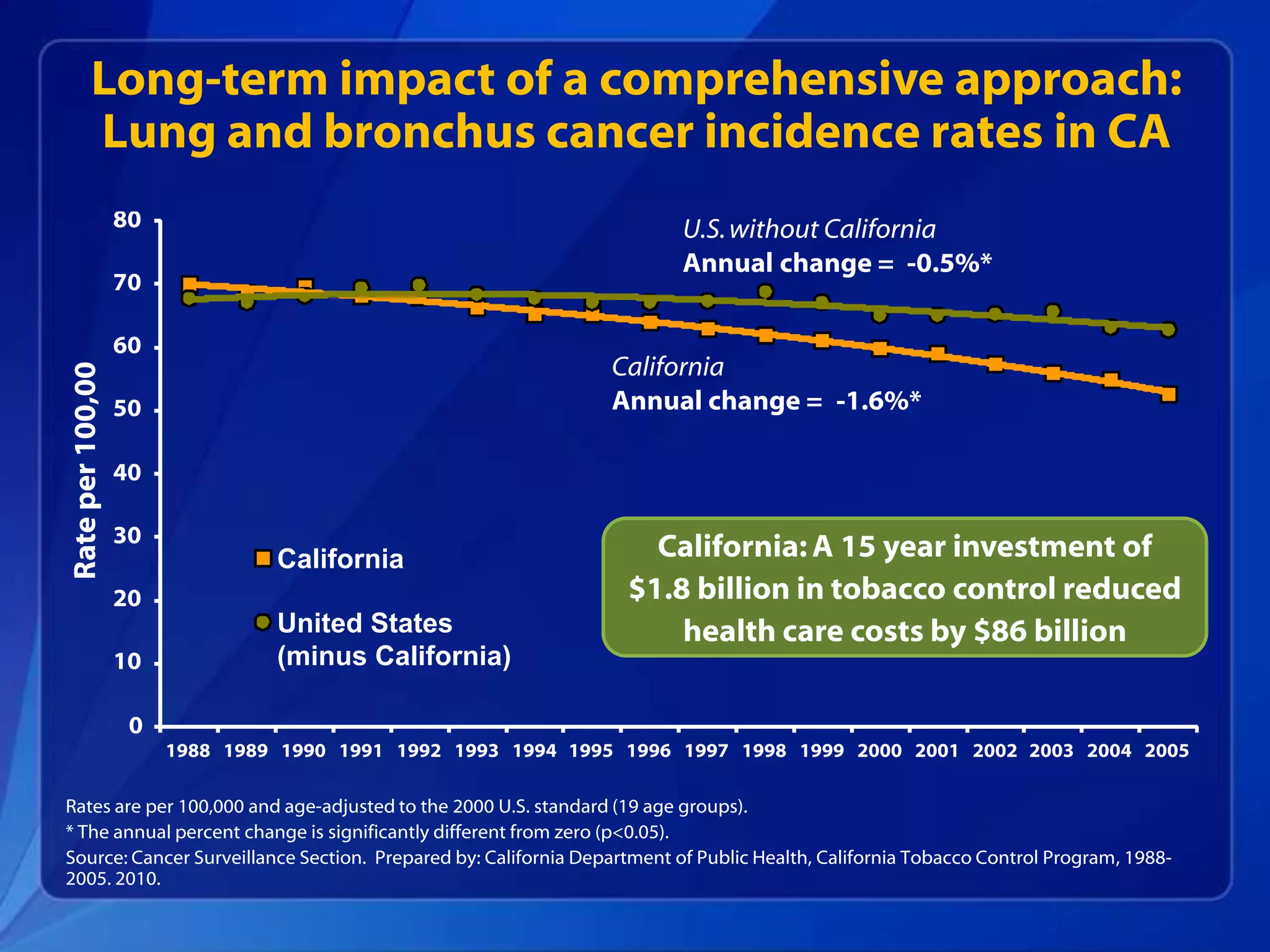
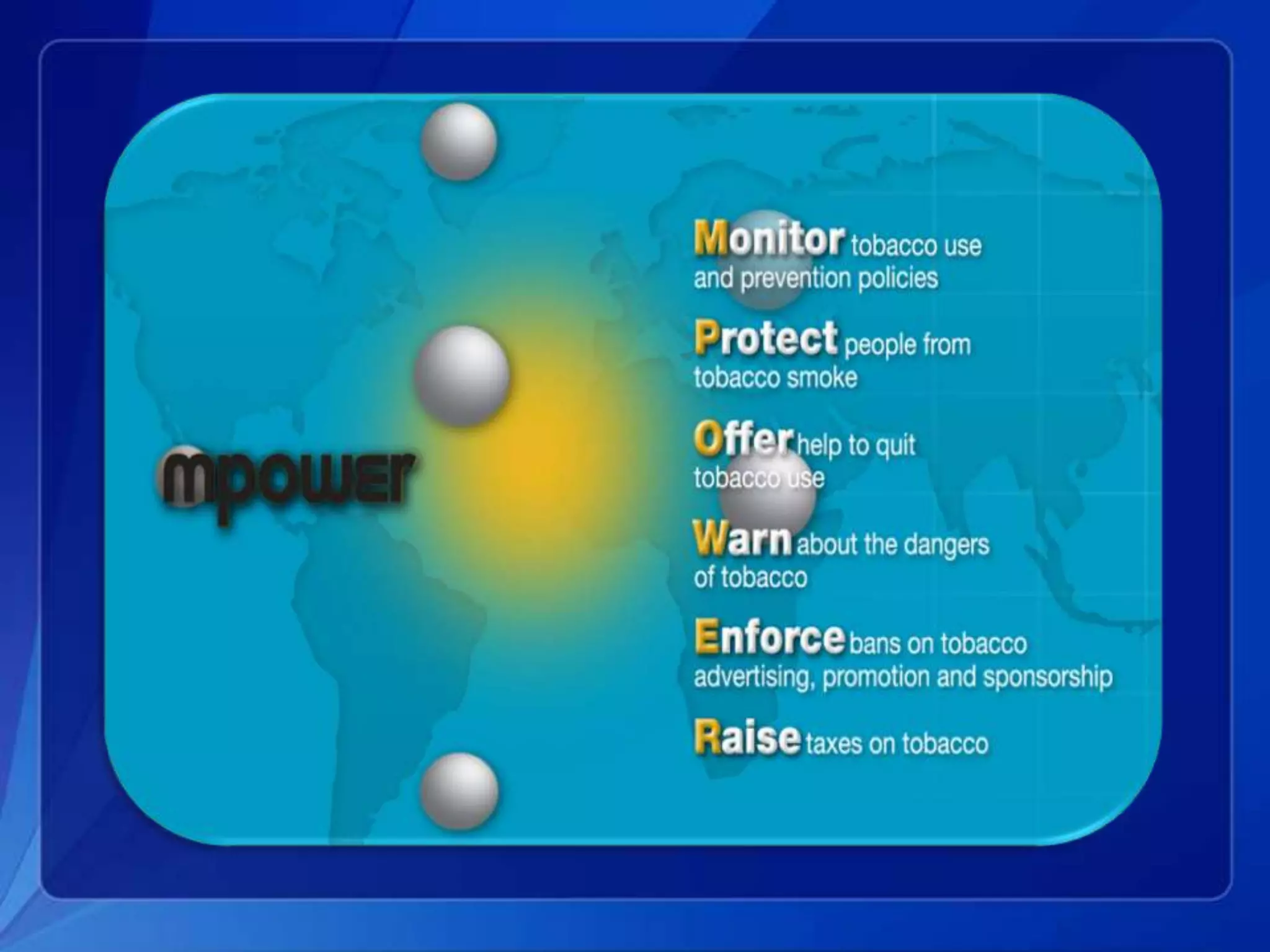
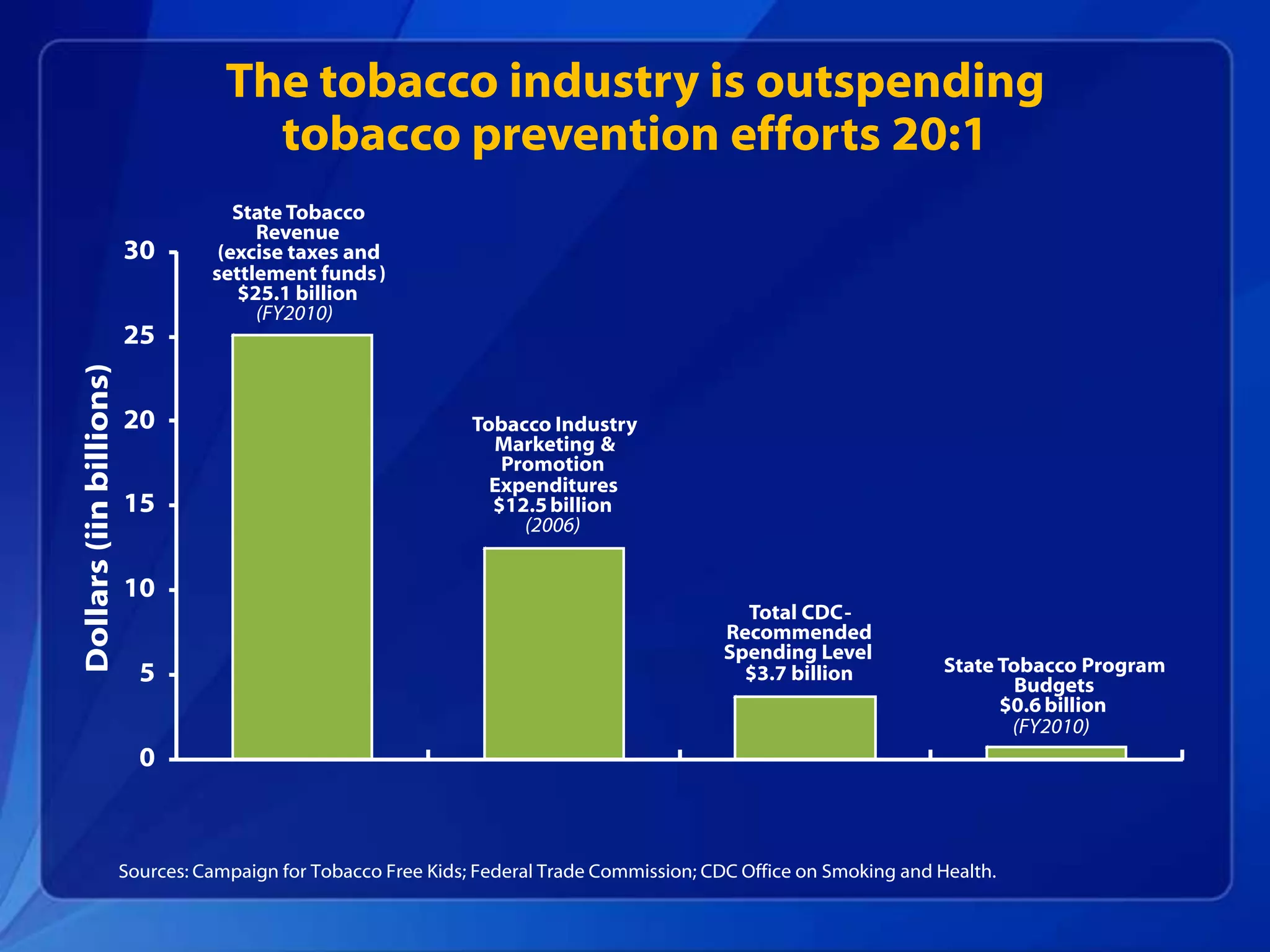
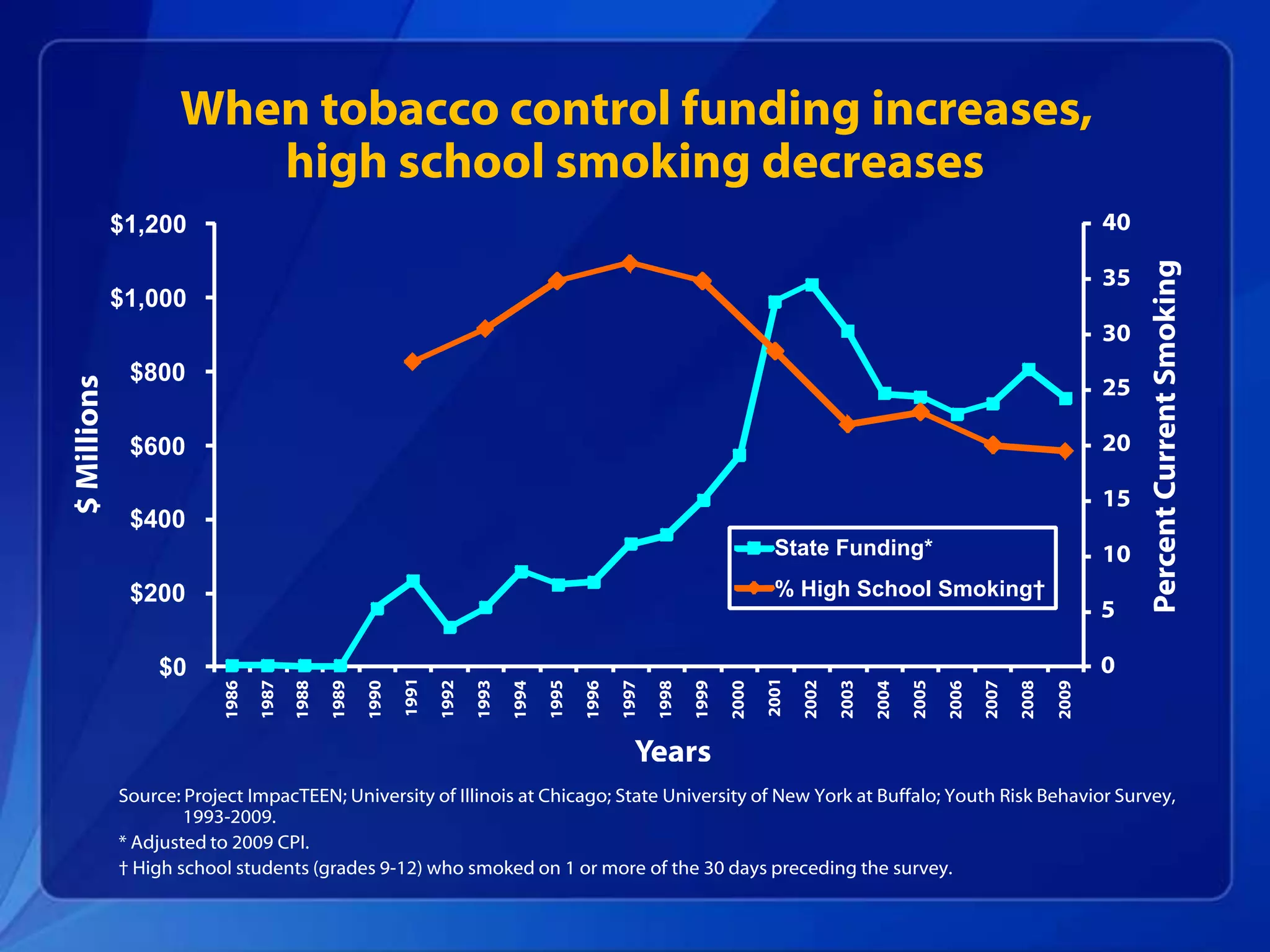
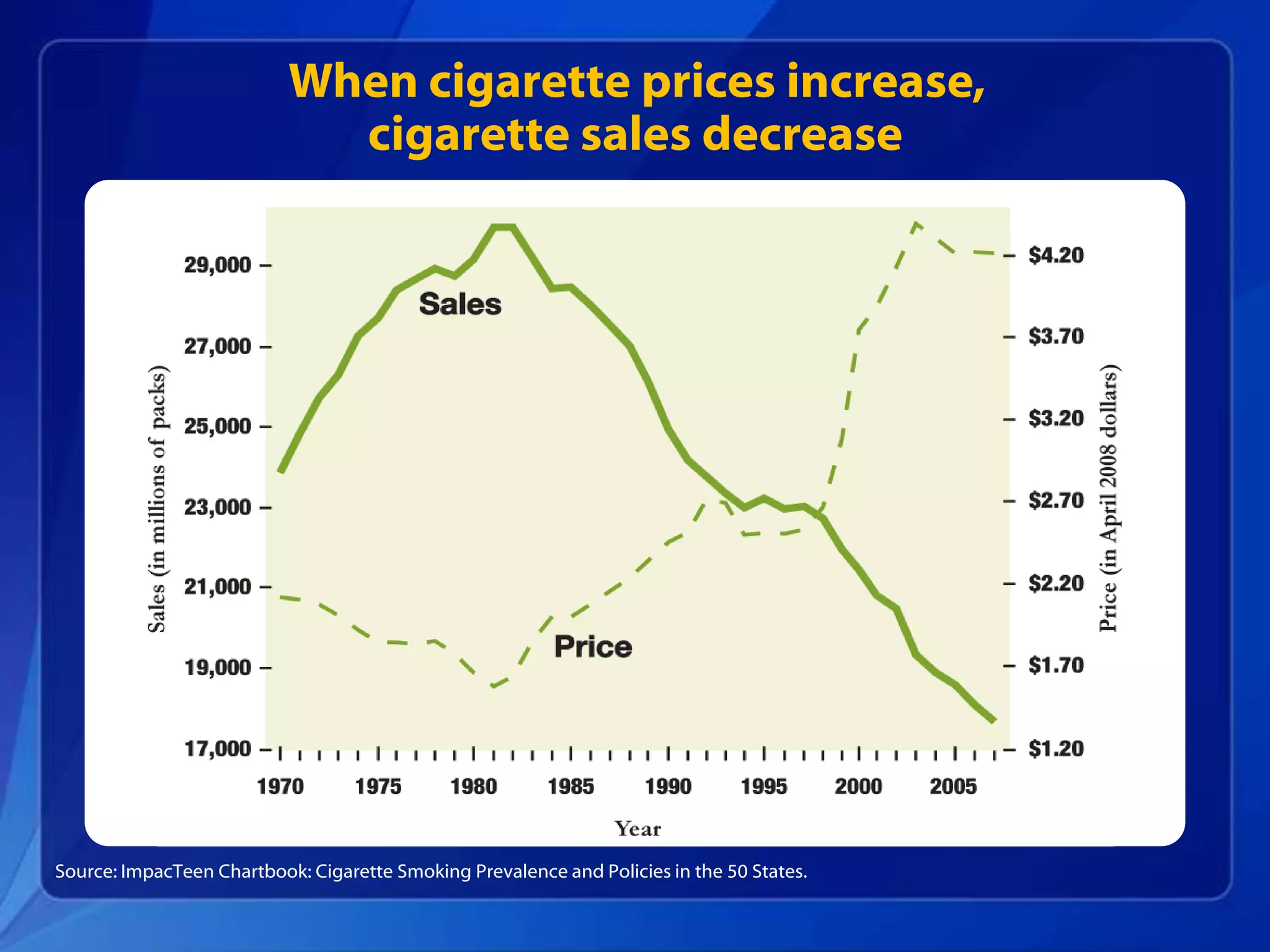
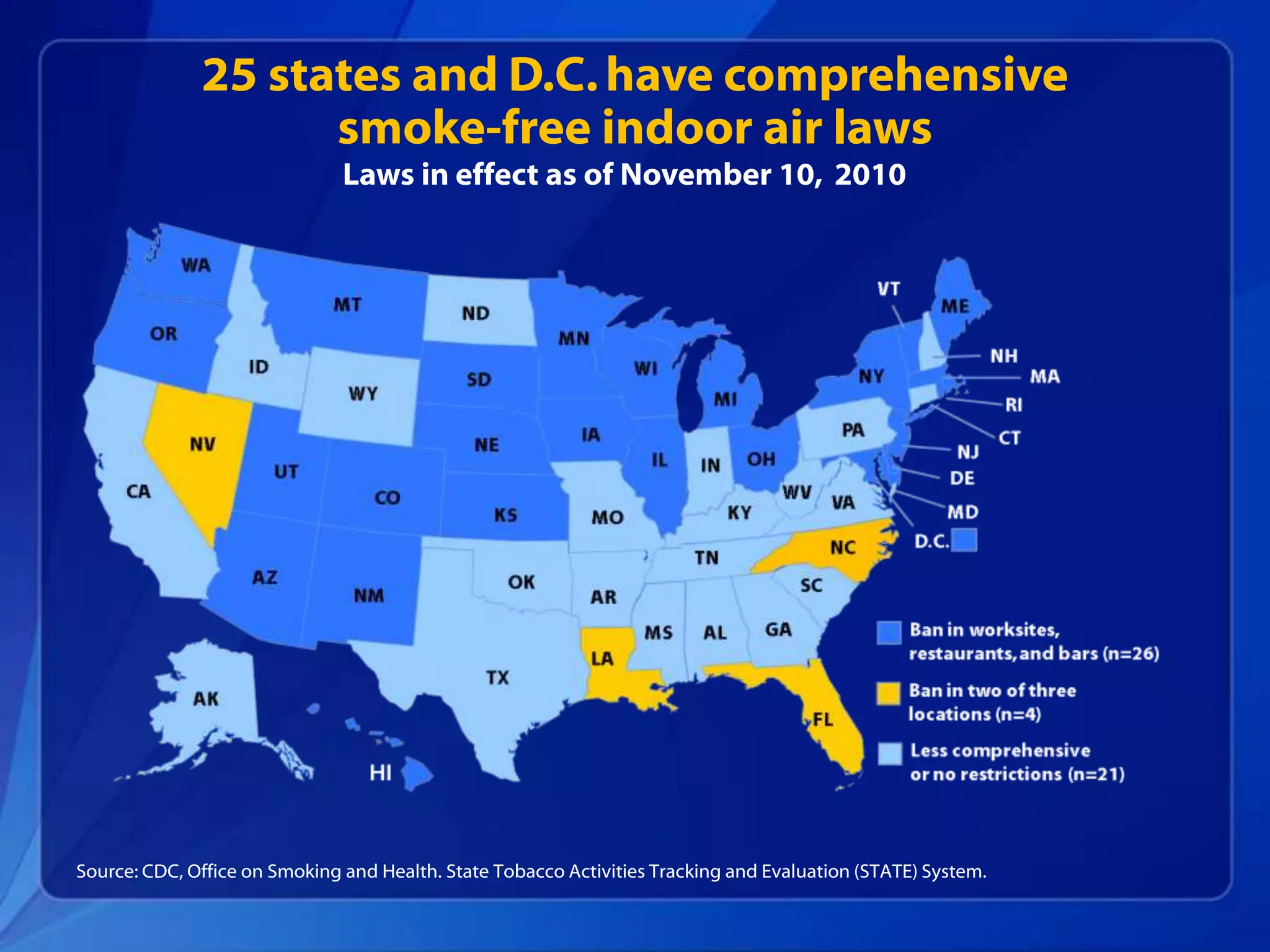
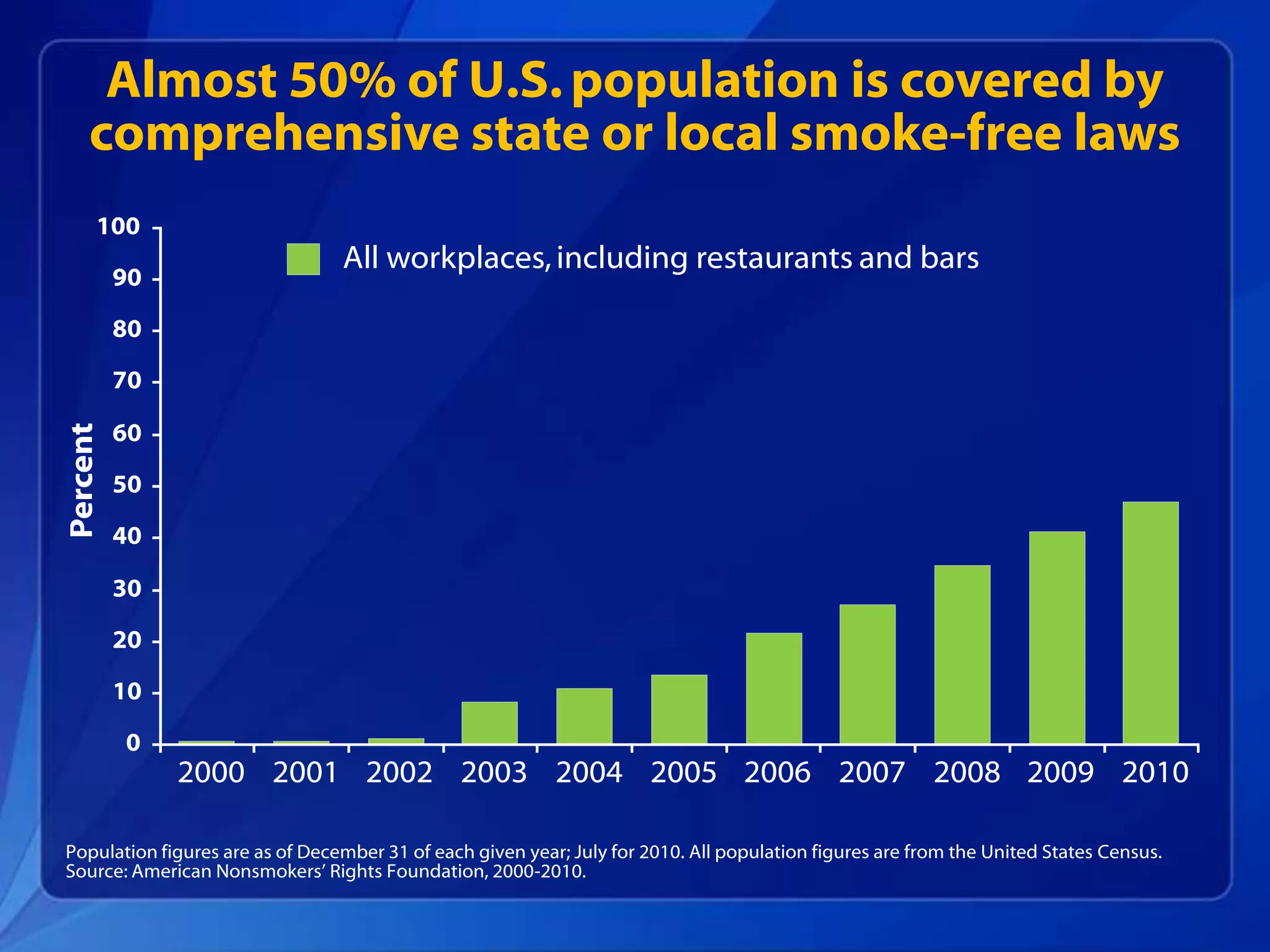
Tobacco use is still the leading preventable cause of death in the U.S., killing over 440,000 Americans each year. While smoking rates have declined, progress has stalled in recent years. Comprehensive tobacco control programs that increase tobacco taxes, implement smoke-free laws, fund anti-smoking media campaigns, and increase access to cessation services have been shown to effectively reduce smoking rates and the health burdens and economic costs of tobacco use. However, more remains to be done as the tobacco industry continues to outspend tobacco control efforts. Sustained funding and expansion of comprehensive tobacco control programs nationwide are needed to continue making progress toward creating a tobacco-free generation.