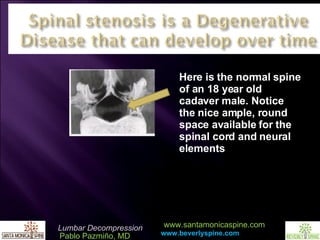
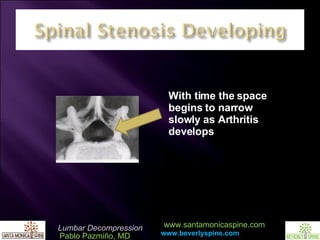




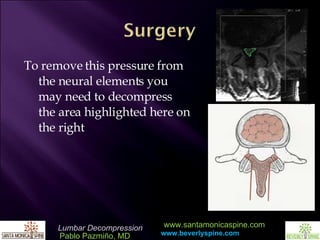
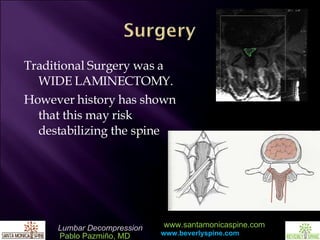
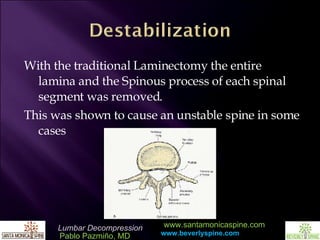



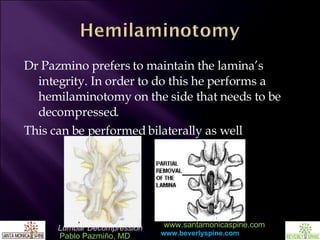
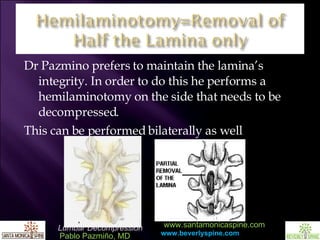
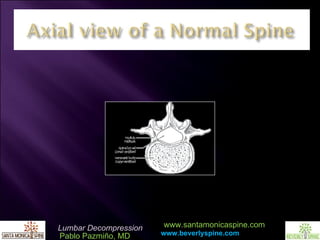
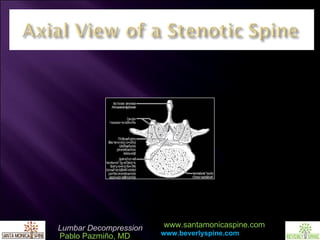

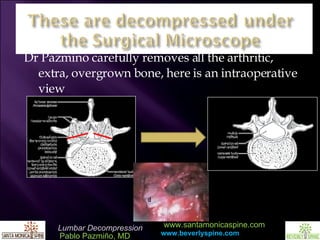



Dr. Pablo Pazmiño discusses the normal spine structure and the effects of arthritis on spinal health, emphasizing the importance of a foundational understanding of MRI imaging in spinal surgery. He outlines the process of minimally invasive lumbar decompression surgery, detailing the techniques used to avoid destabilizing the spine, including hemilaminotomy and careful decompression. The presentation concludes with an invitation for referrals for consultations related to lumbar decompression.











































































