Downloaded 371 times



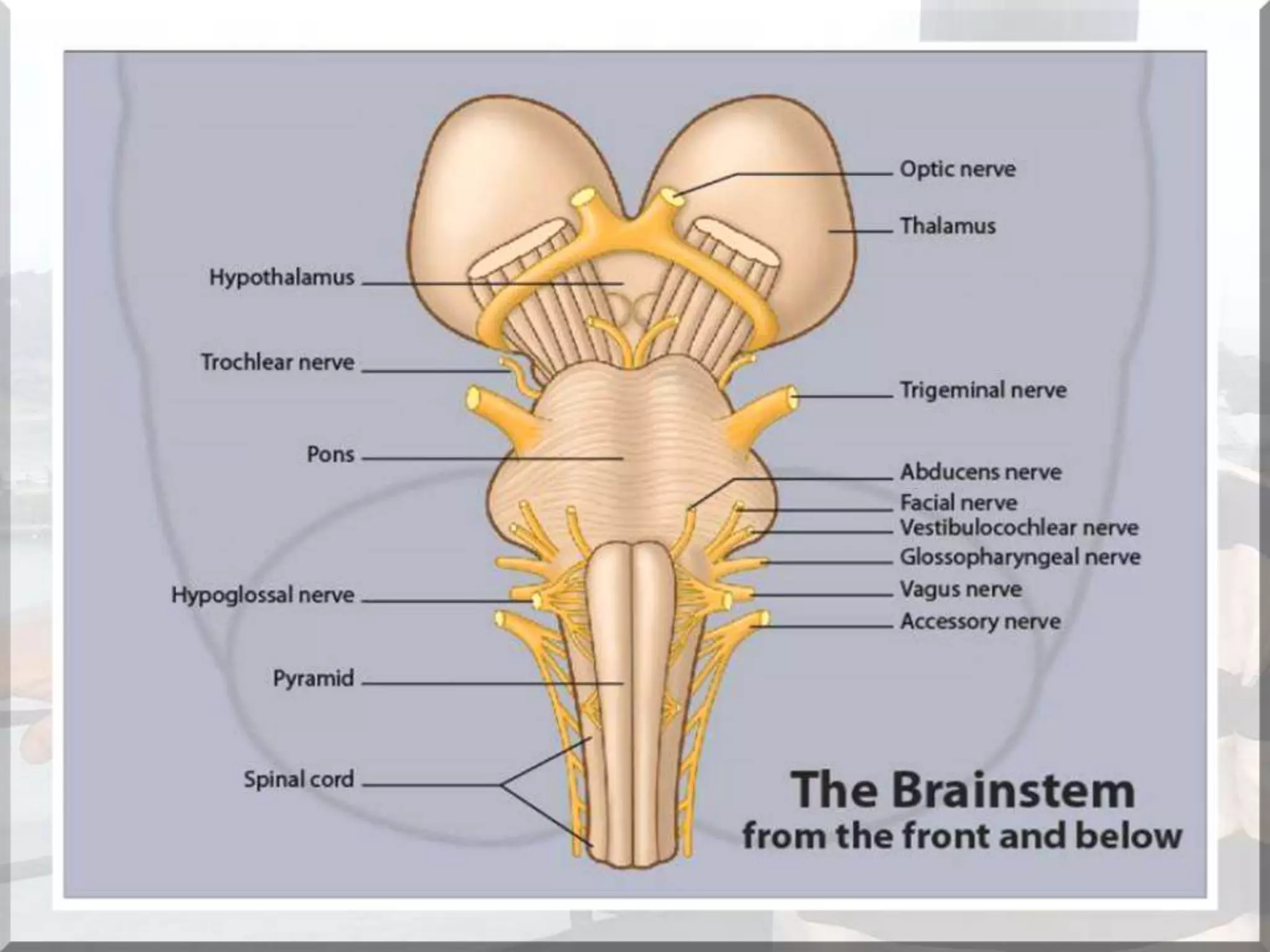
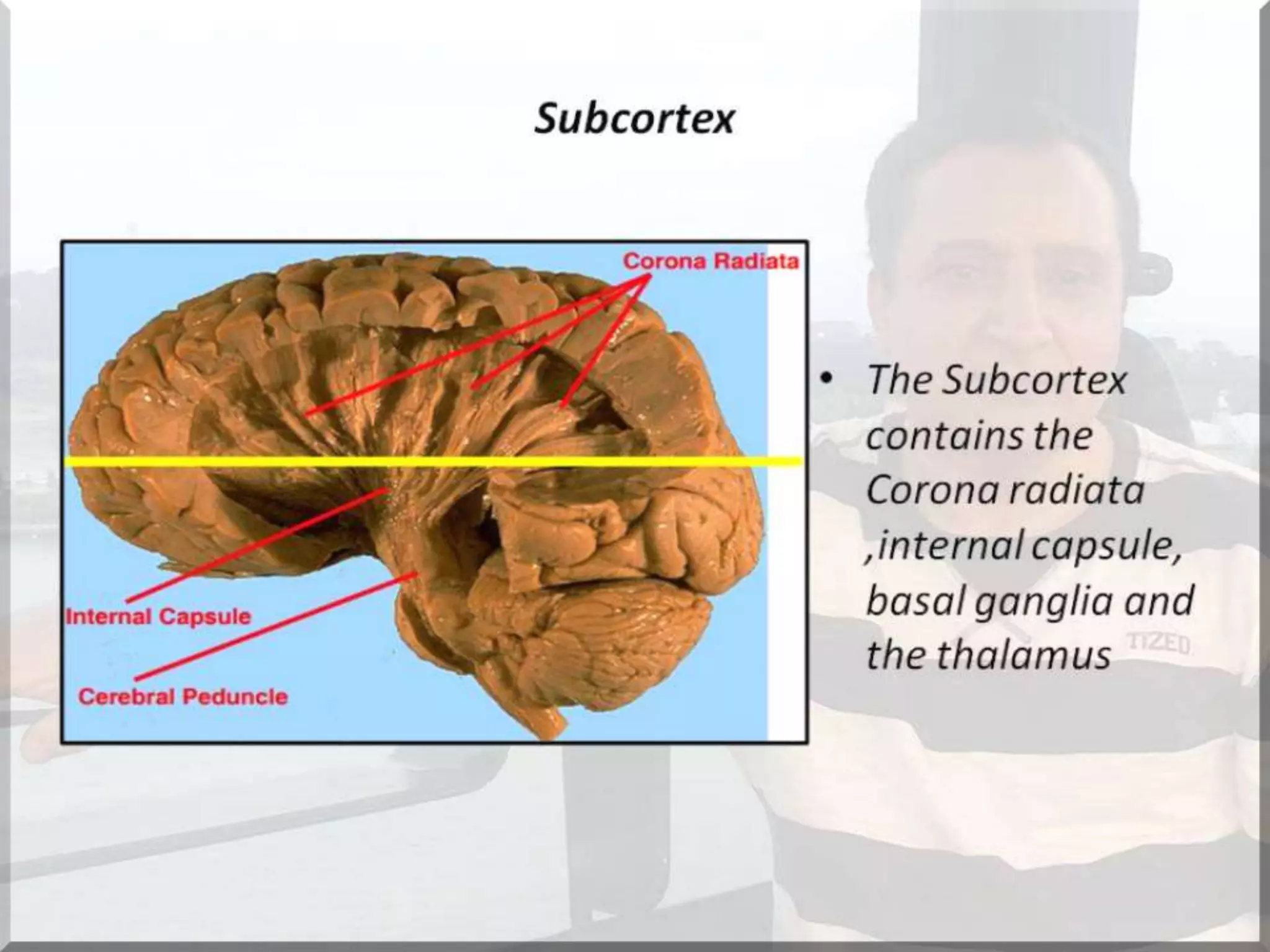

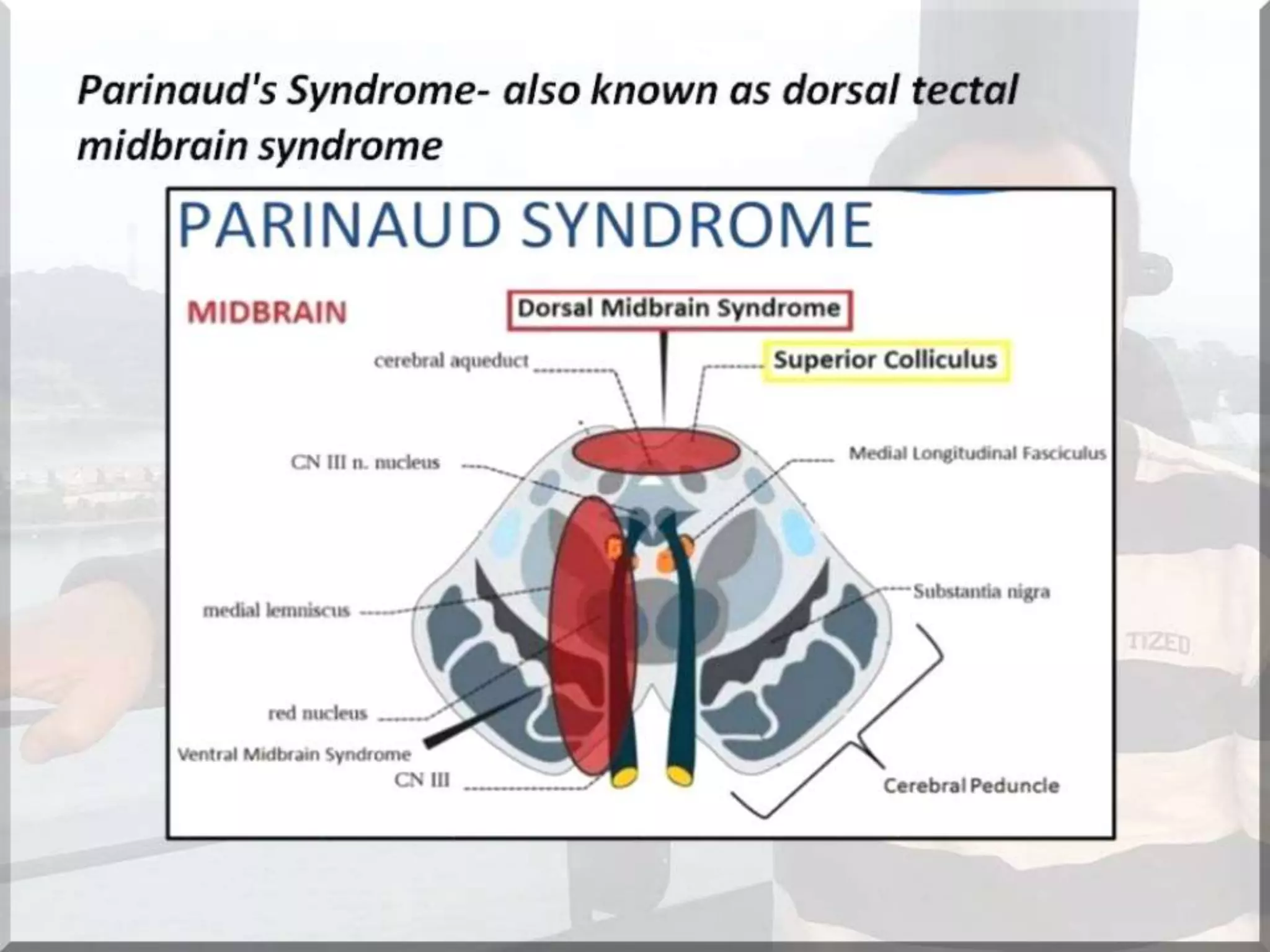
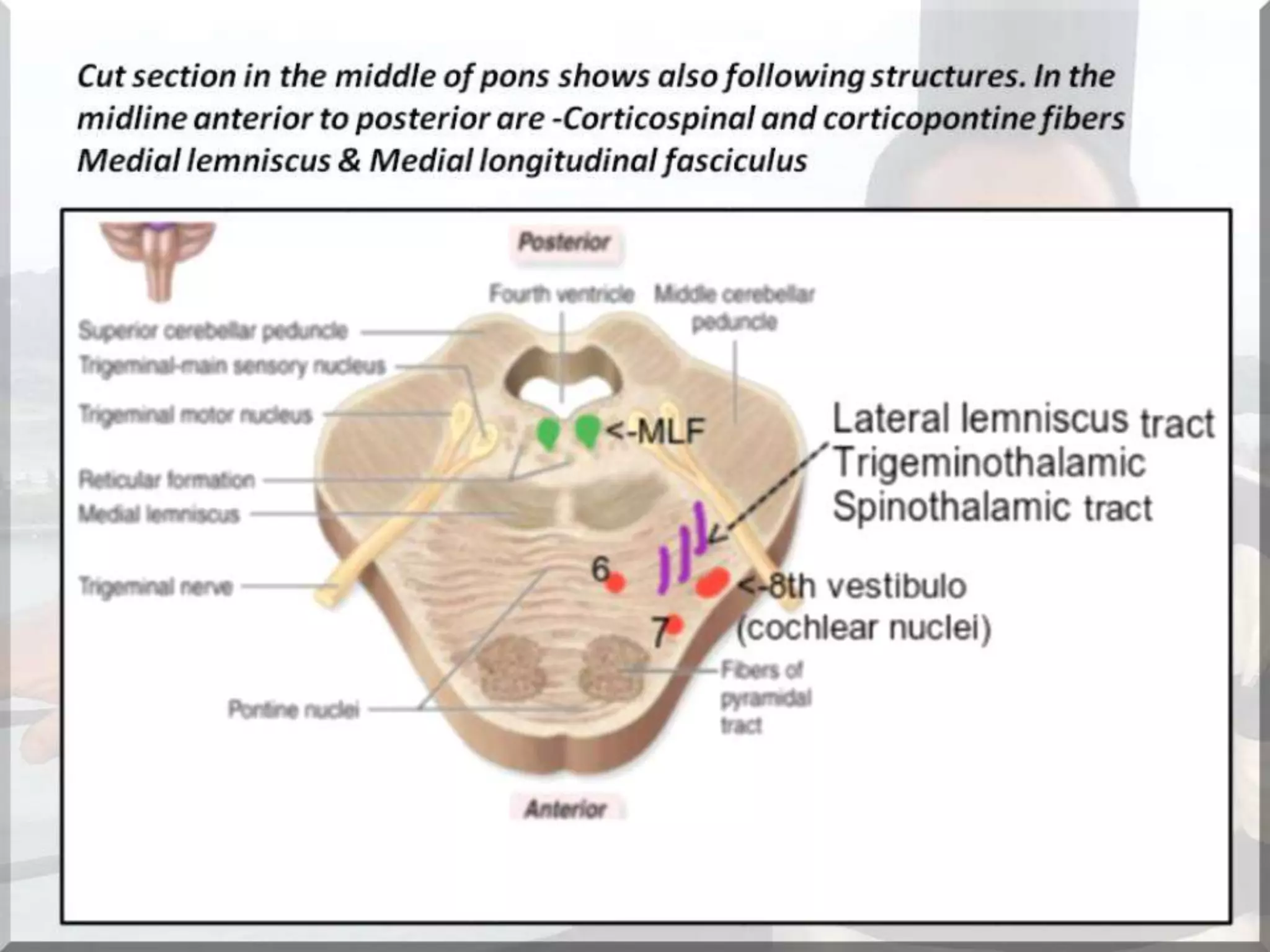
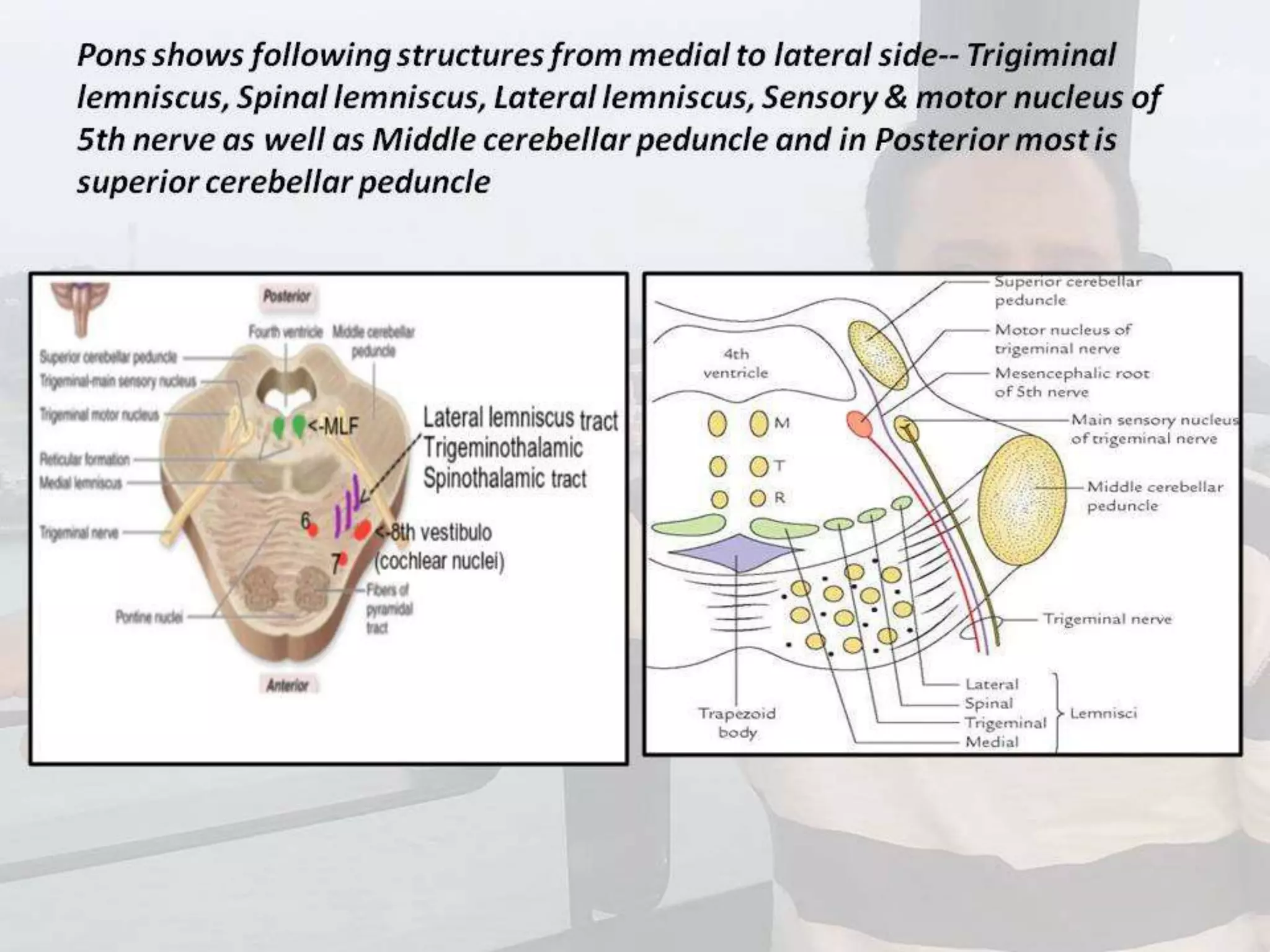
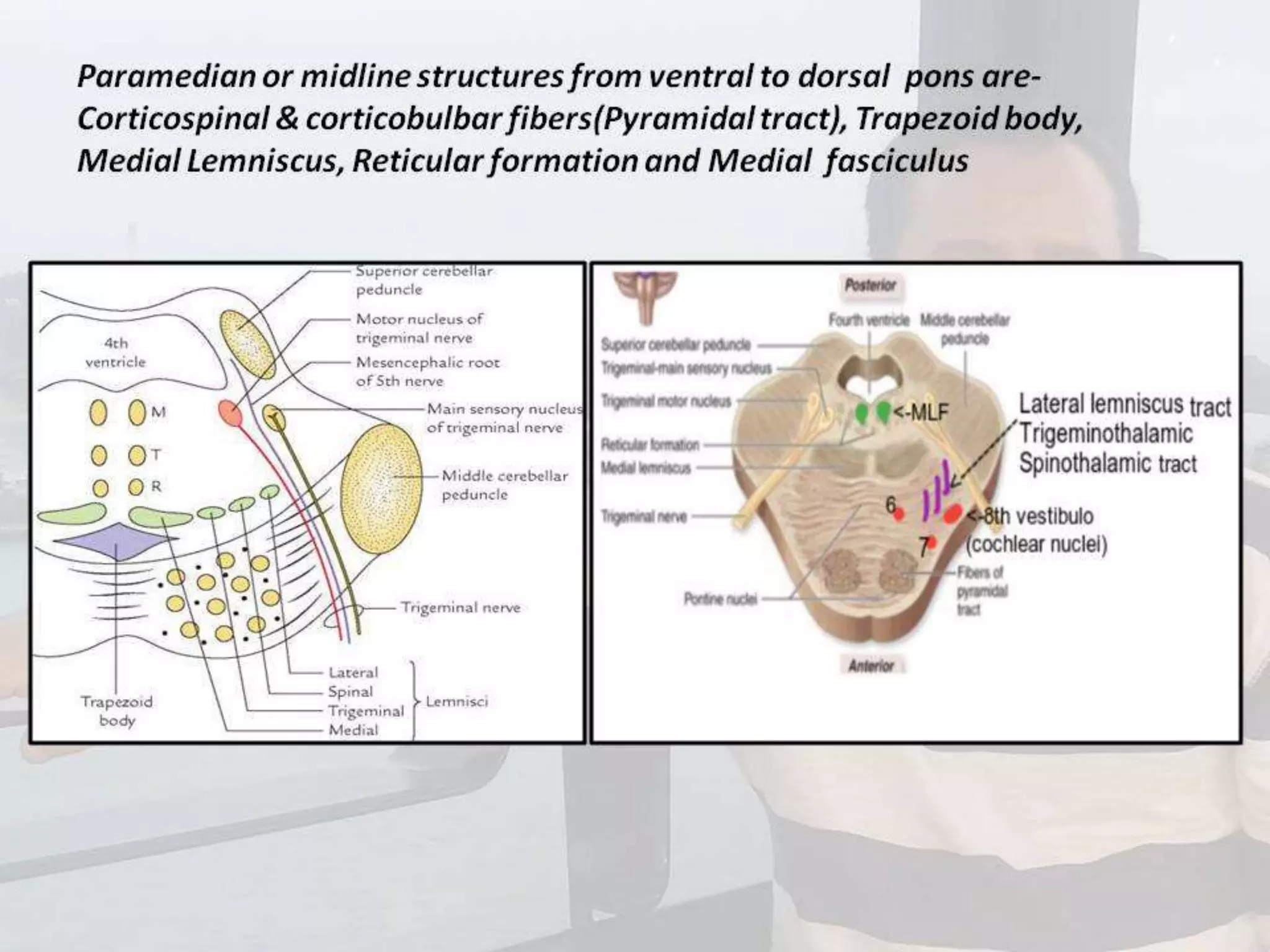
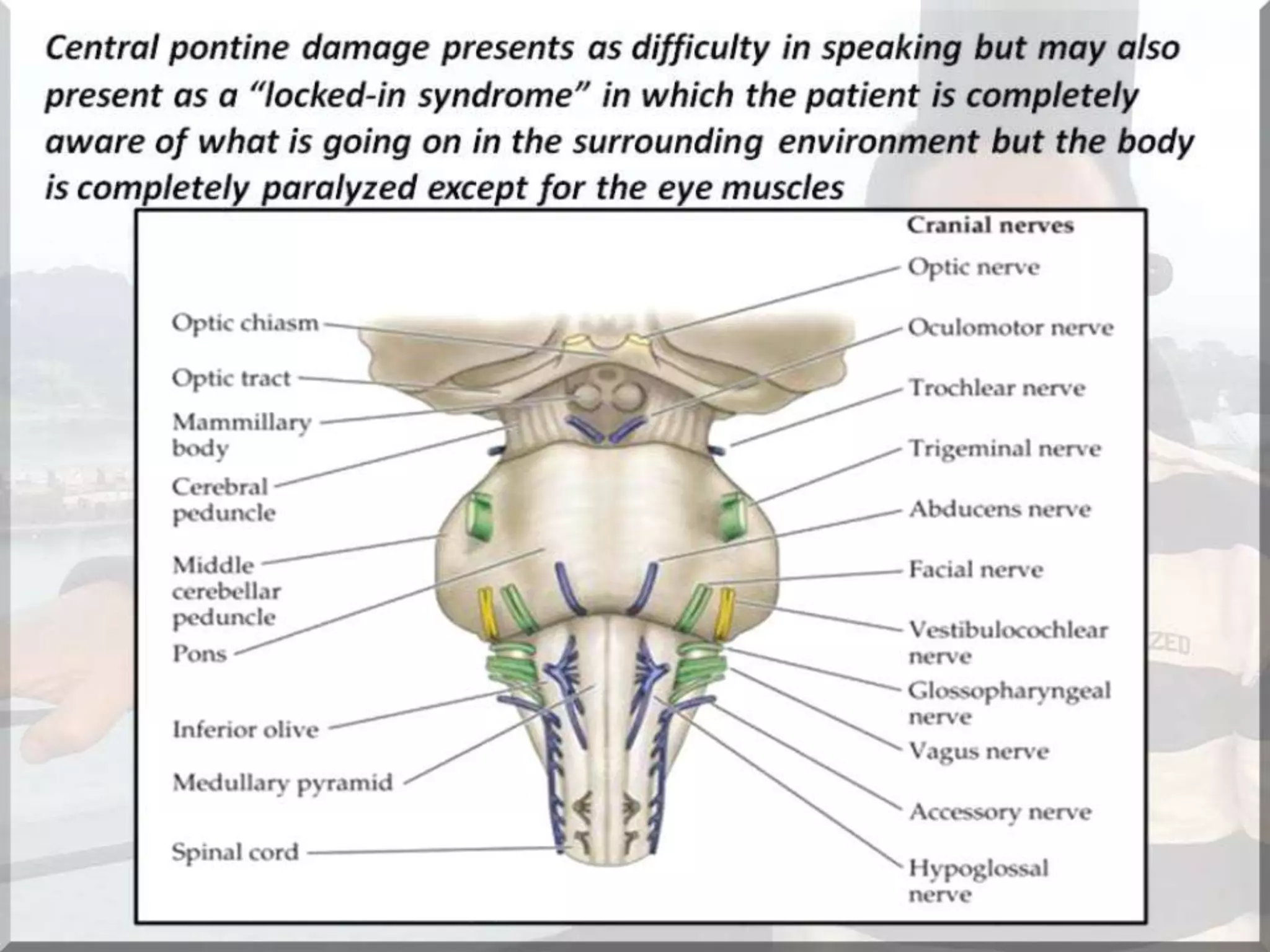
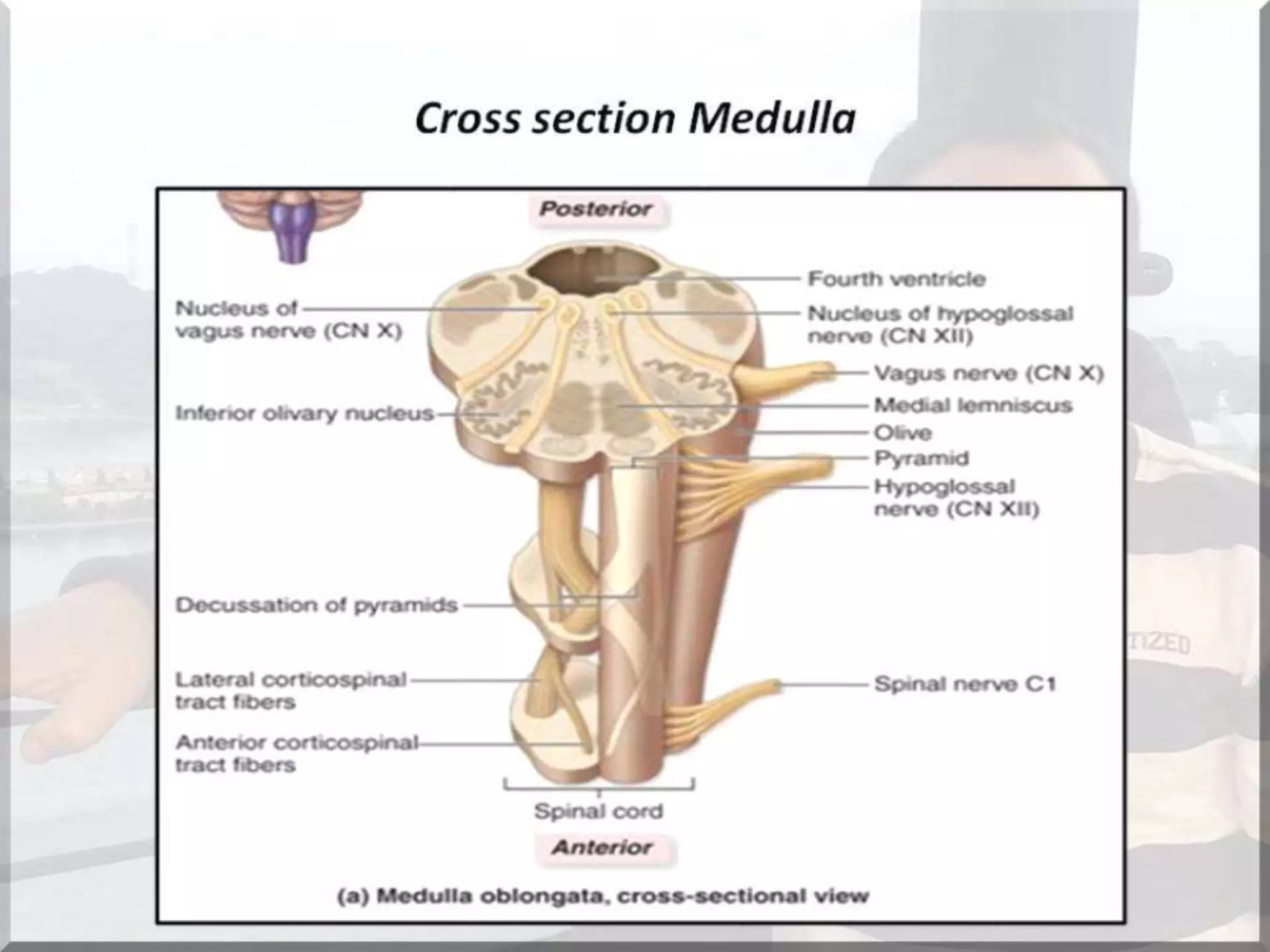

The document discusses the brainstem, which consists of the midbrain, pons, and medulla. It refers to a previous lecture on brain lesion localization and includes information on subcortex and internal capsule in the presentation. The lecture on brainstem lesions builds upon earlier concepts introduced by Prof. Dr. Bashir Ahmed Dar.