Download to read offline
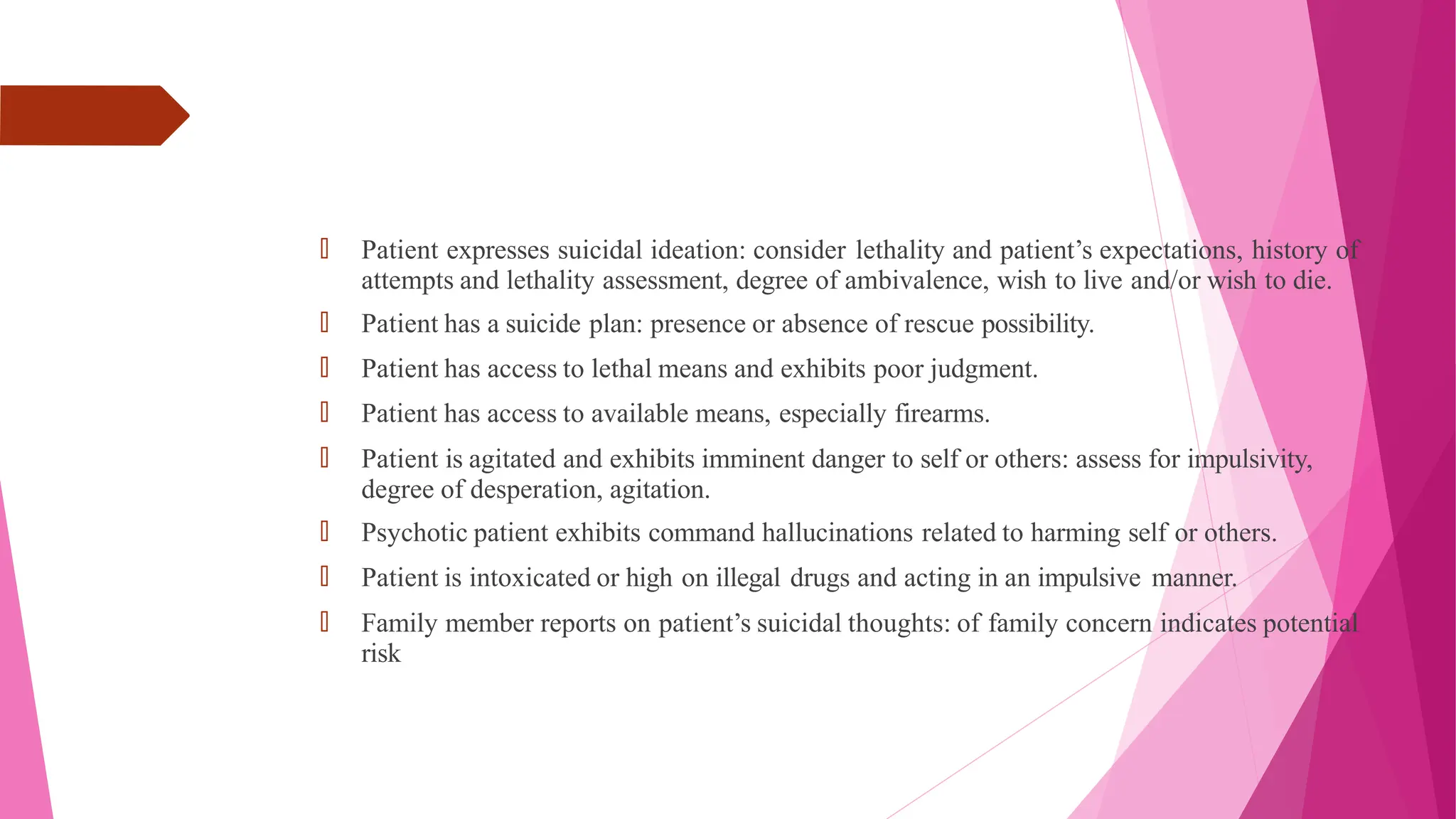
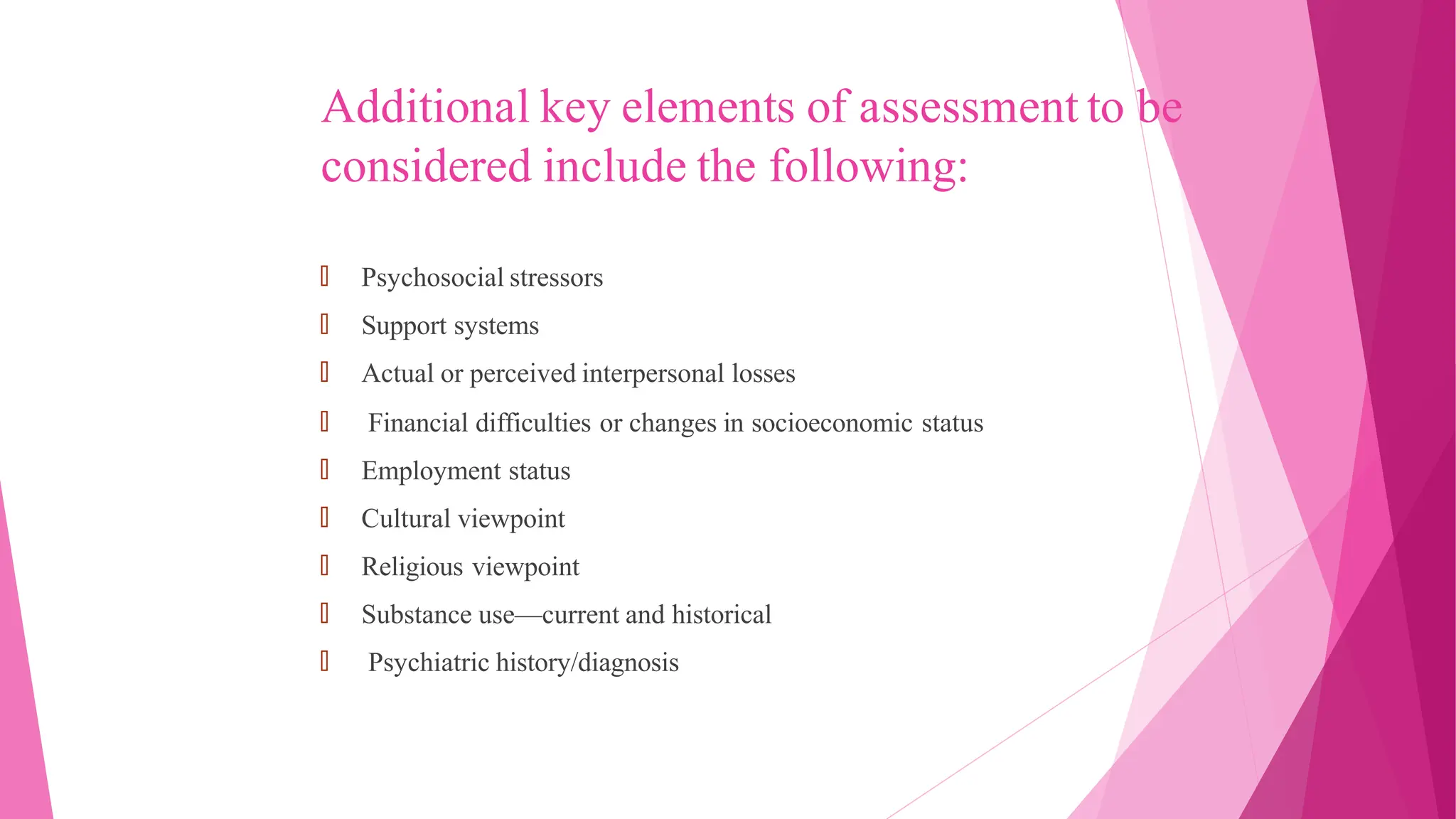
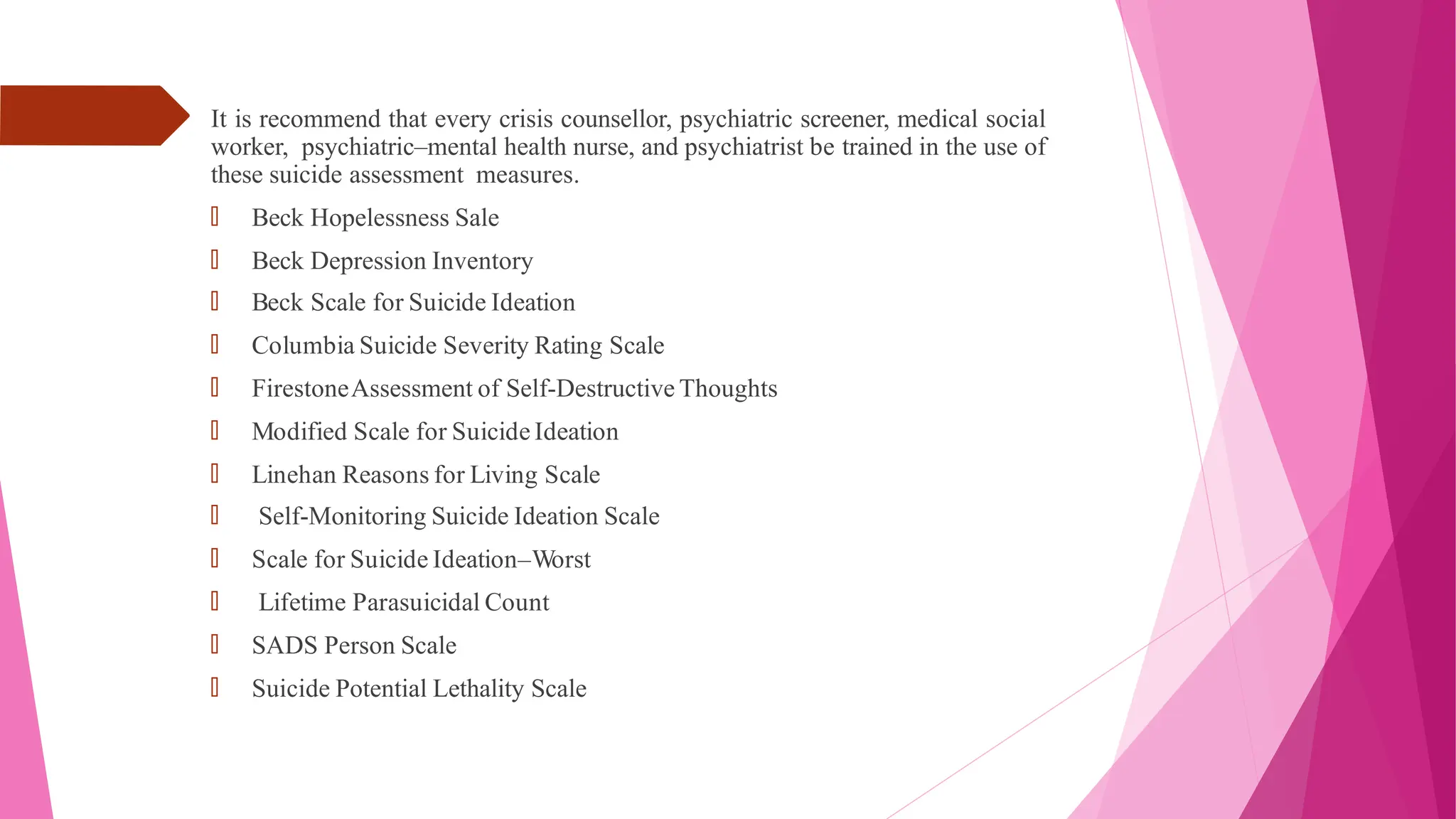
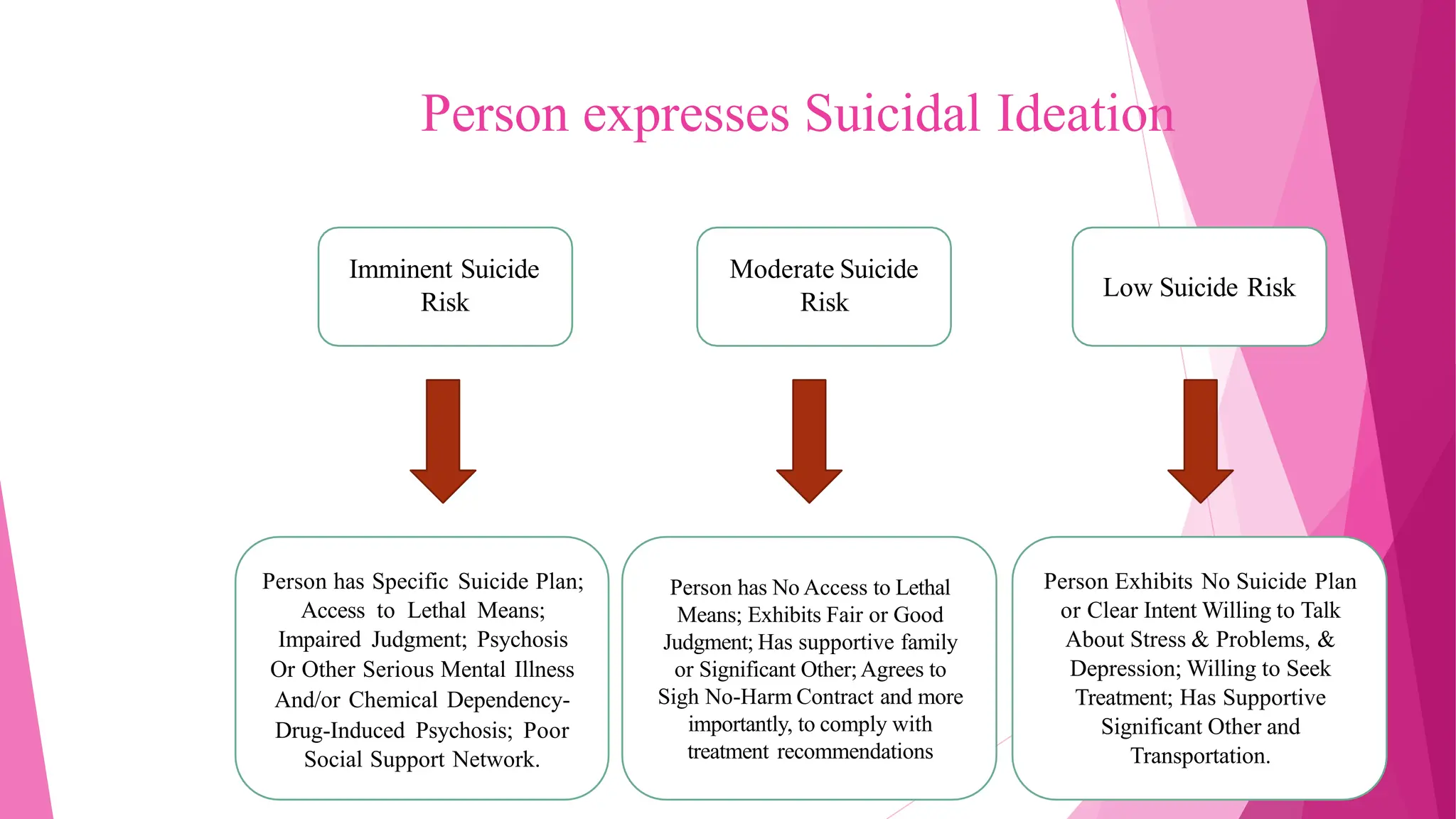


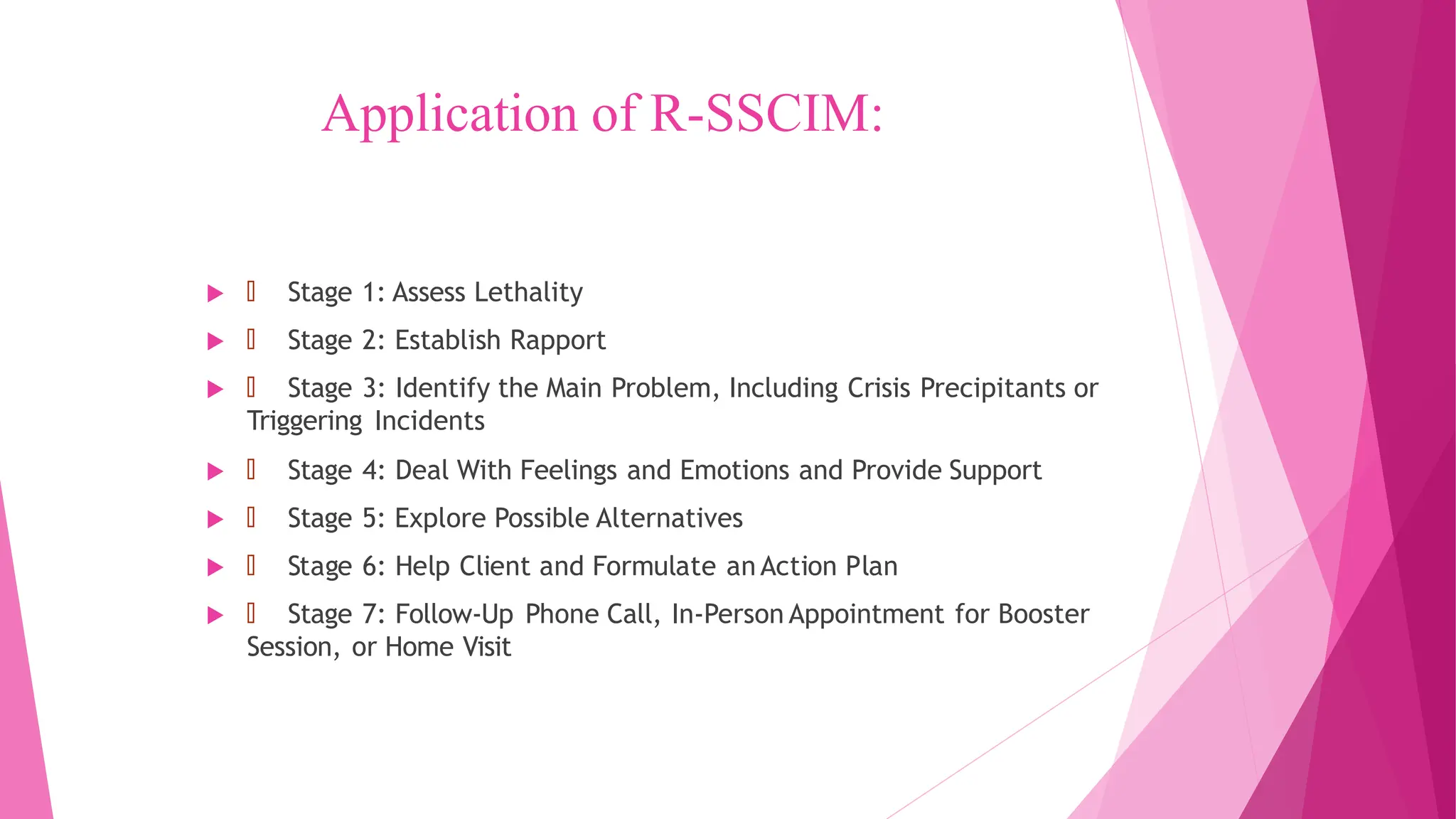




The document discusses lethality assessments and crisis interventions, particularly in the context of suicidal ideation and risk evaluation. It outlines various factors that contribute to assessing someone's risk of suicide, emphasizes the importance of crisis intervention, and details the structured Robert's seven-stage model for crisis intervention. Case studies illustrate the assessment process and the intervention steps taken to support individuals in crisis.























































































