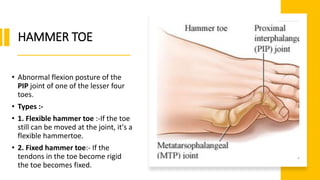
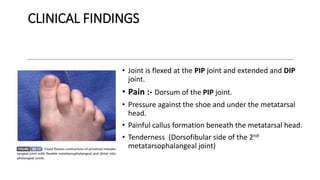
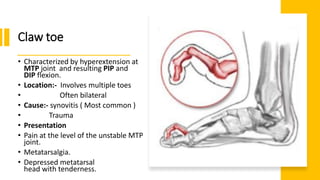
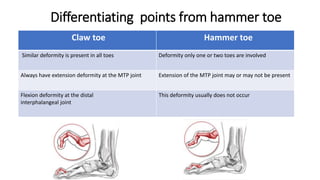
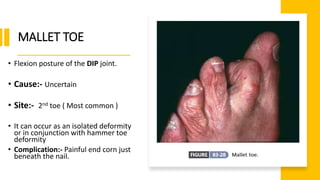
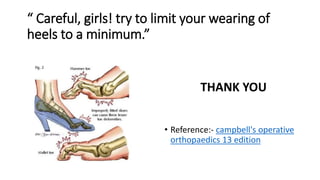
This document discusses various abnormalities of the lesser toes including hammer toe, claw toe, mallet toe, and corns. Hammer toe is an abnormal flexion of the PIP joint. Claw toe involves hyperextension of the MTP joint and flexion of the PIP and DIP joints. Mallet toe is a flexion deformity of the DIP joint. Corns are hyperkeratotic lesions caused by pressure and friction. Treatment options discussed include padding, strapping, manipulation, and surgical procedures such as resection and tendon transfers depending on the specific abnormality.