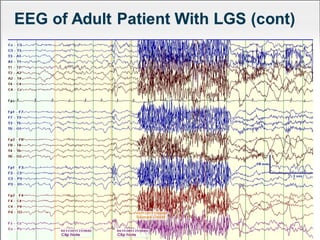
Lennox Gastaut Syndrome (LGS) is a severe childhood epileptic encephalopathy characterized by multiple seizure types including tonic-atonic seizures. It typically has an onset between ages 3-8 and causes cognitive impairment. Treatment involves identifying the syndrome and selecting effective therapies like clobazam, felbamate, lamotrigine, and rufinamide while avoiding treatments that can worsen seizures. The ketogenic diet and vagus nerve stimulation may also provide benefit.