


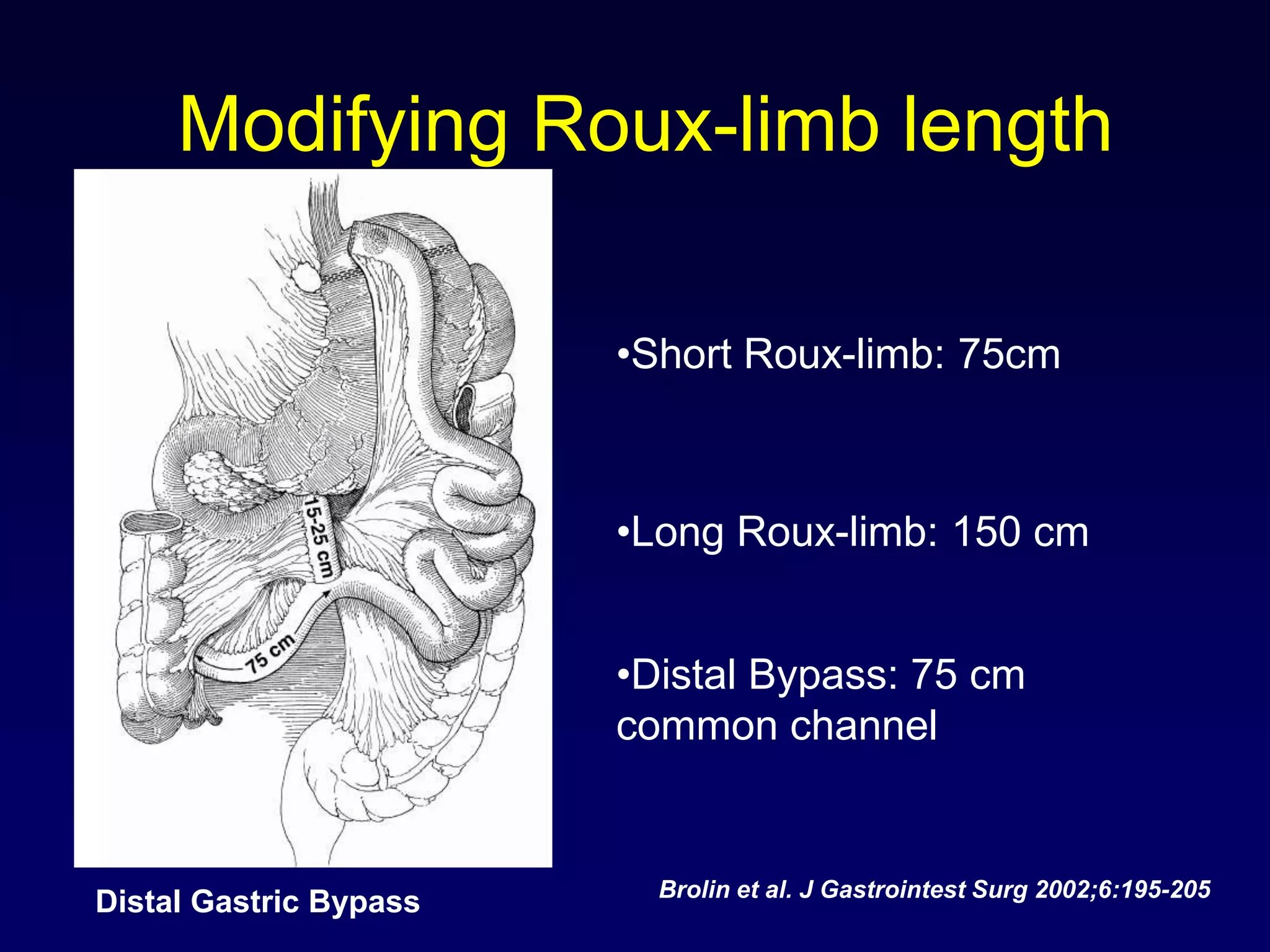
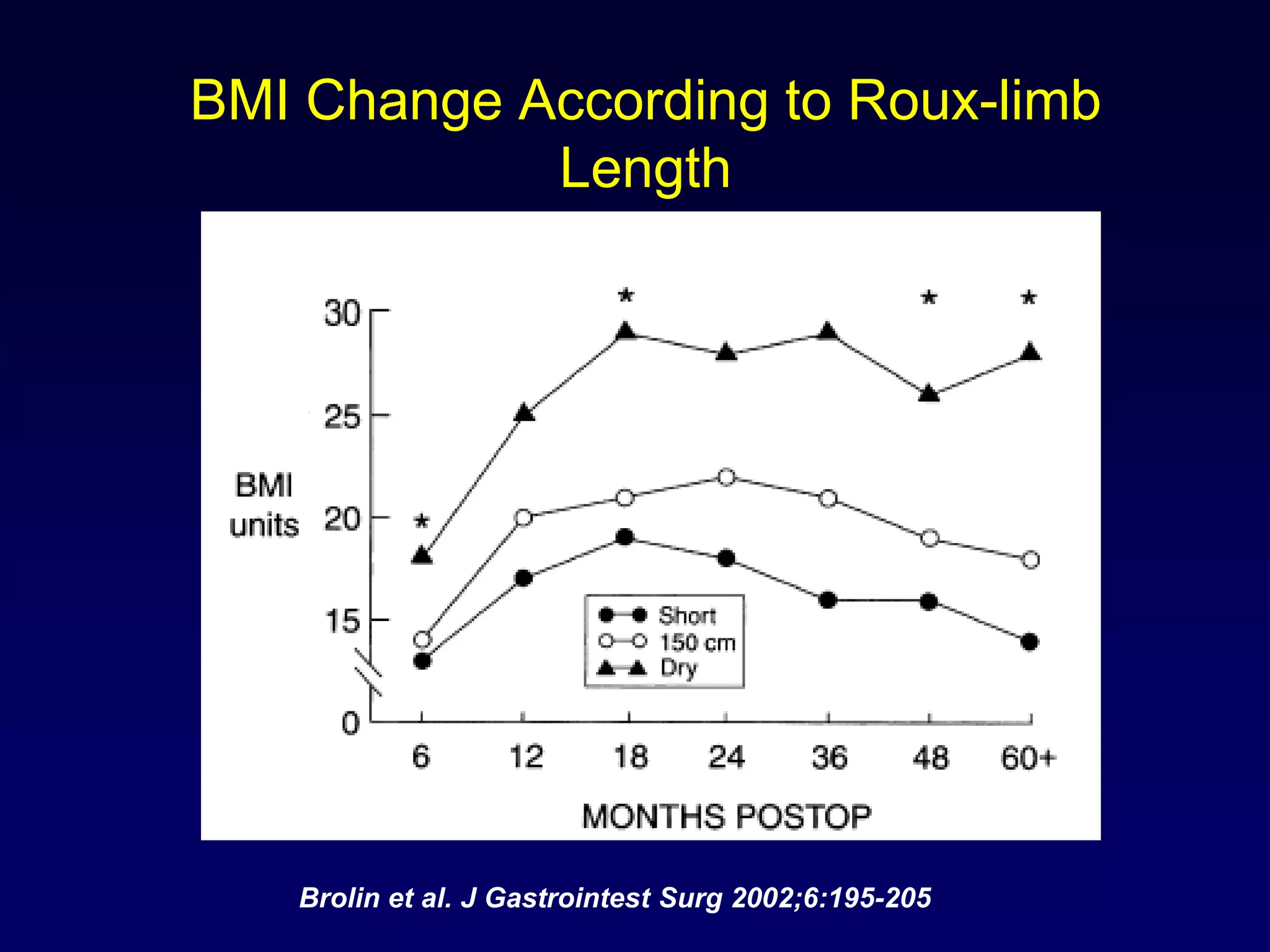
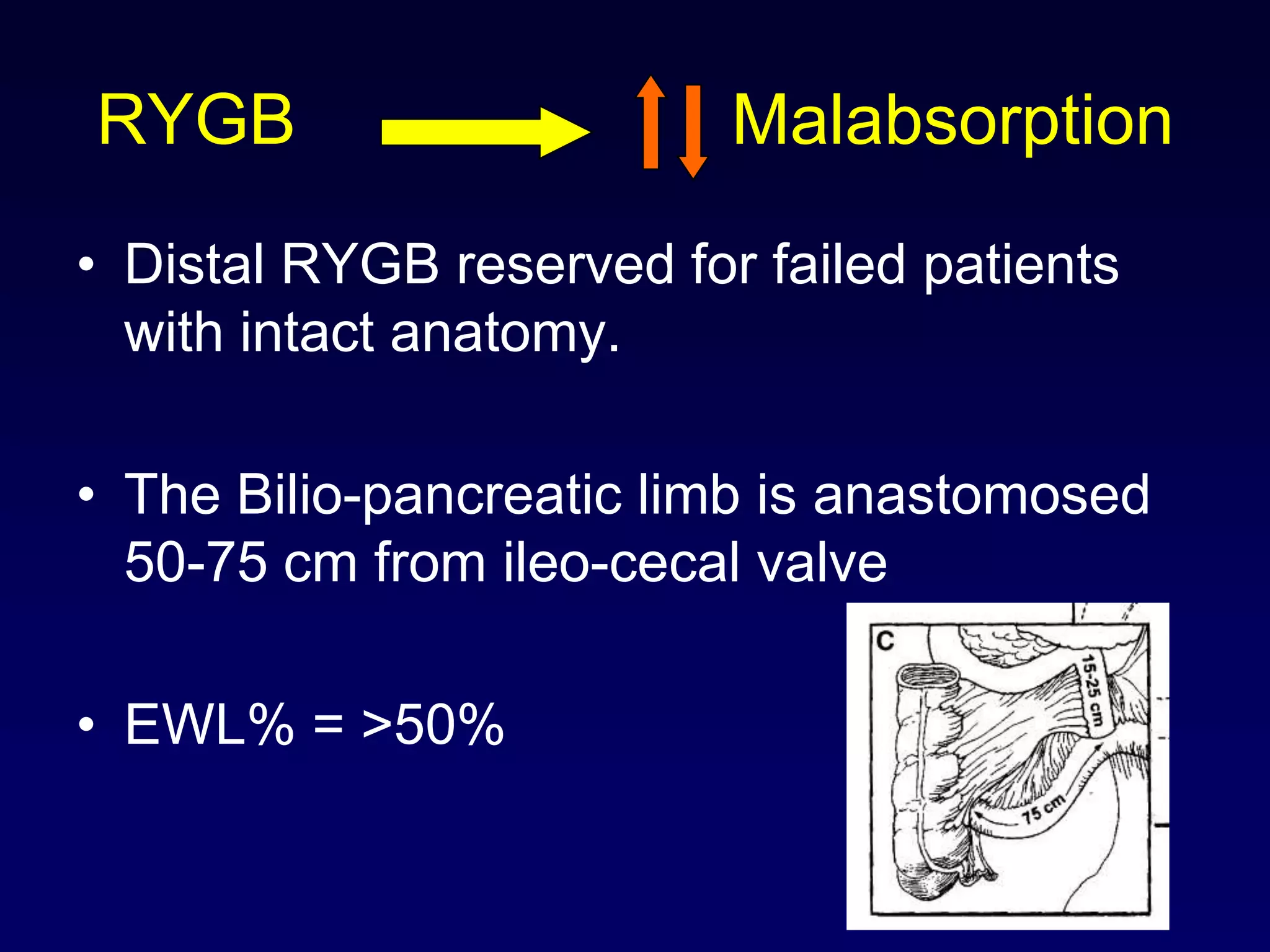
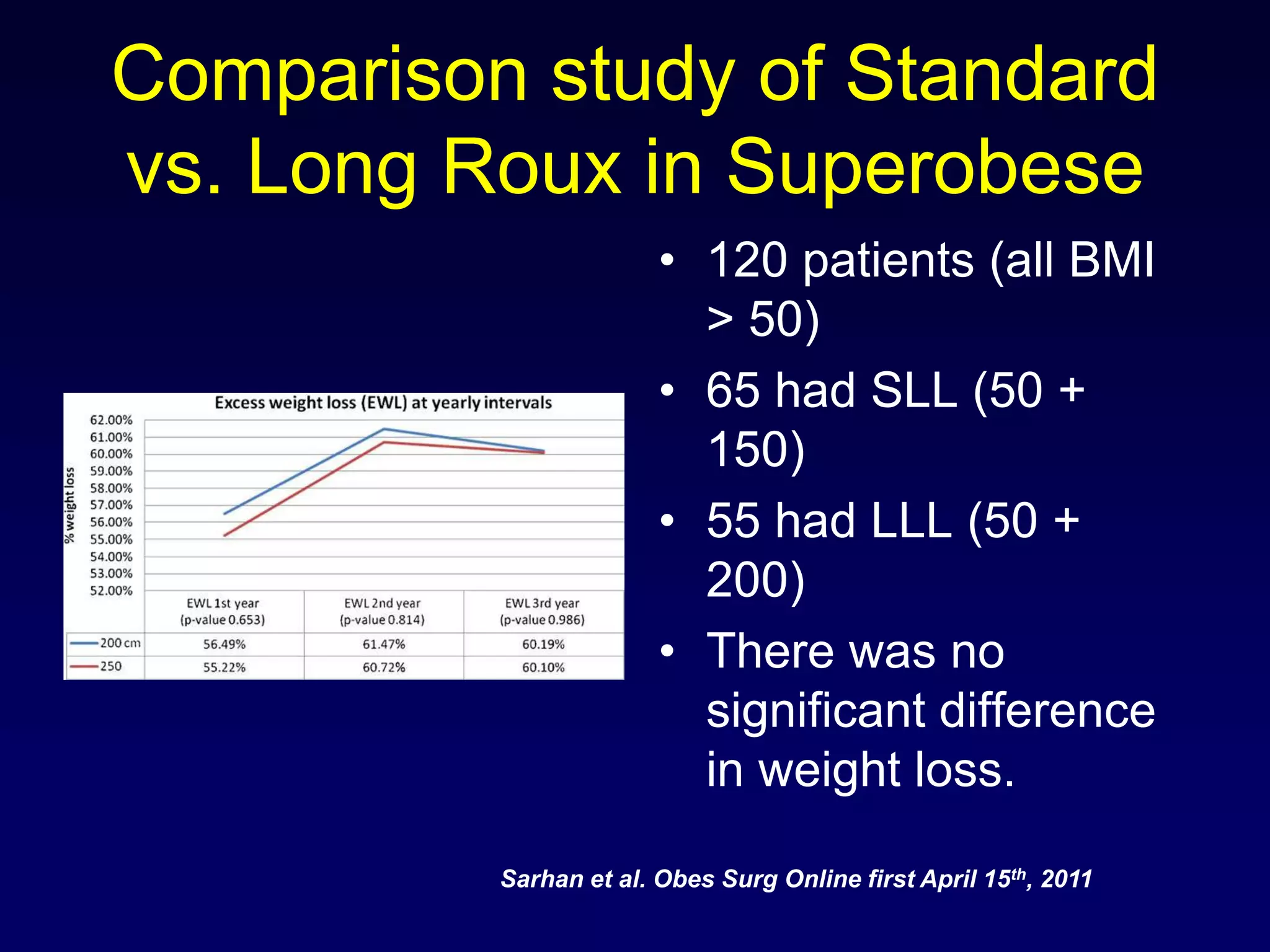

This document discusses how the length of the Roux limb in gastric bypass surgery may impact outcomes. It notes that while longer Roux limbs between 150-200 cm do not significantly impact weight loss, even more distal bypass with Roux limbs of only 50-75 cm from the ileocecal valve can cause greater weight loss but also increases risks of nutritional deficiencies. The document reviews evidence from studies comparing standard to longer or more distal Roux limb lengths and their effects on weight loss and complications.























































































