
Downloaded 39 times
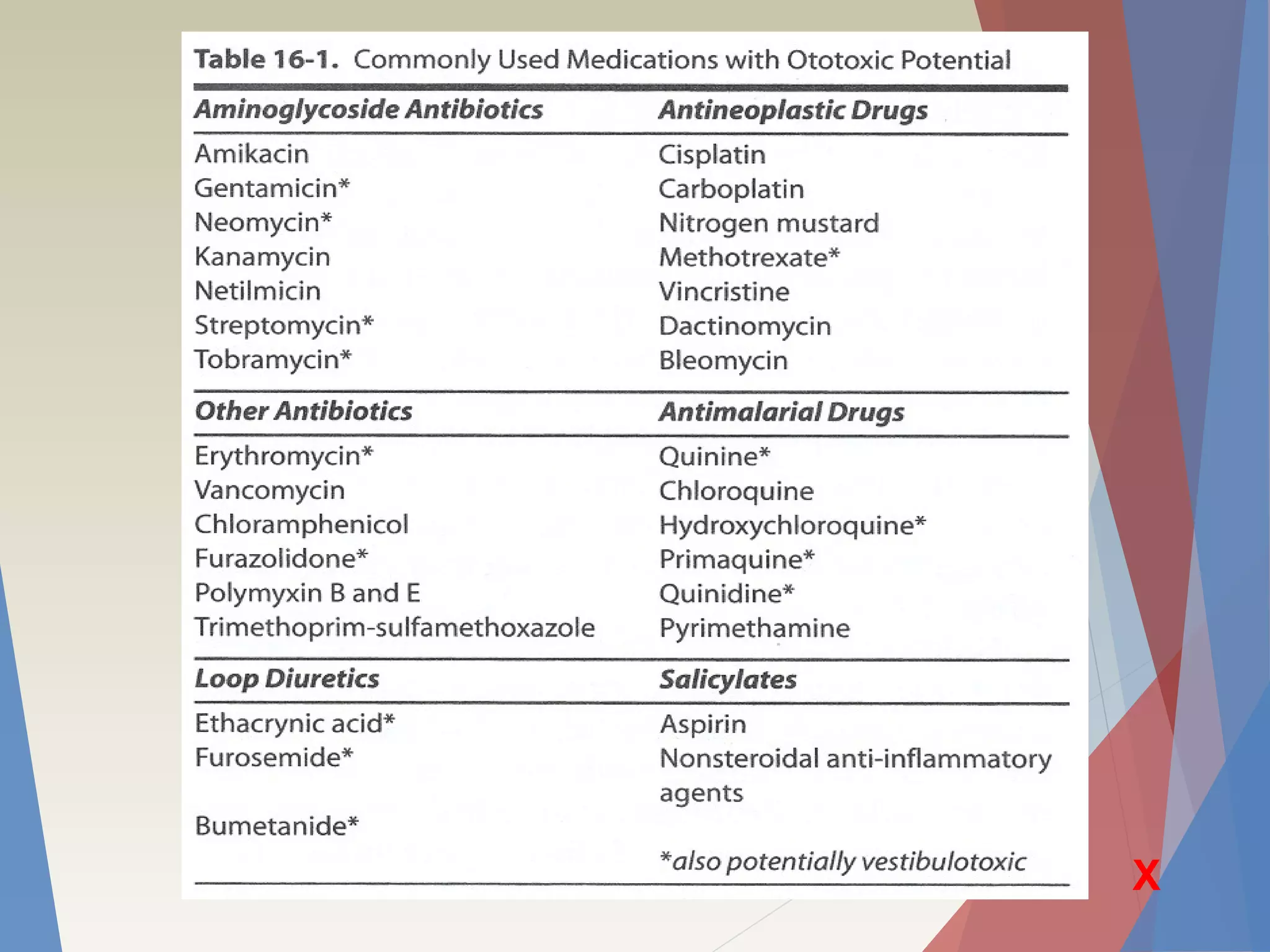
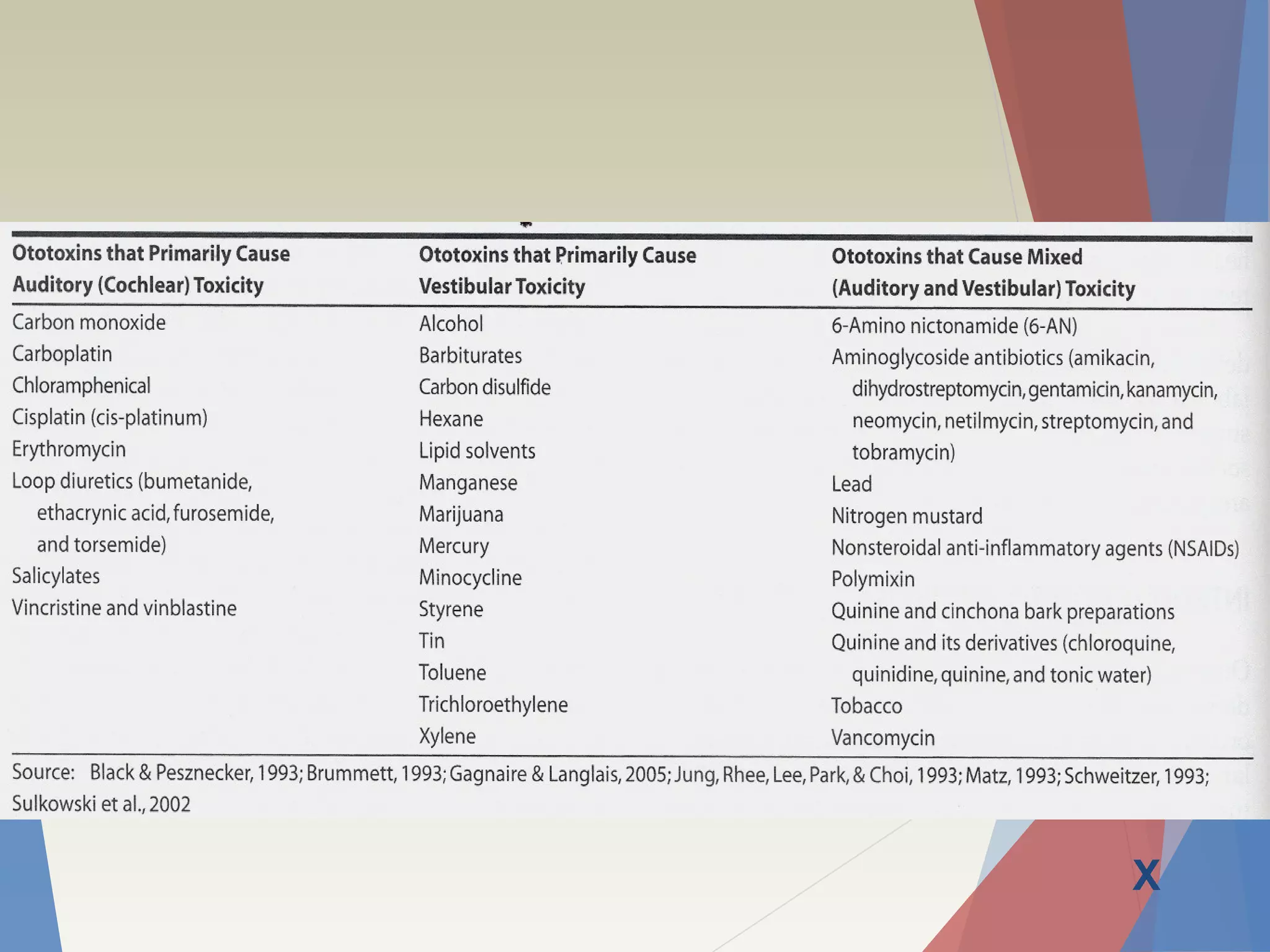
Certain medications like aminoglycoside antibiotics and chemotherapy drugs can damage hearing and balance by harming delicate inner ear cells. Regular audiometric monitoring above 8 kHz, where hearing is lost first, is the most effective way to detect this potentially preventable ototoxicity early. Protective strategies are being studied to allow safer use of these important drugs.











































![OTOTOXICITI [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ototoxicitiautosaved-220601192630-412c784c-thumbnail.jpg?width=640&height=640&fit=bounds)





![Introduction to hearing implairment & cochlear implantation]](https://cdn.slidesharecdn.com/ss_thumbnails/introductiontohearingimplairmentcochlearimplantation-161111054000-thumbnail.jpg?width=640&height=640&fit=bounds)





































