Download to read offline

















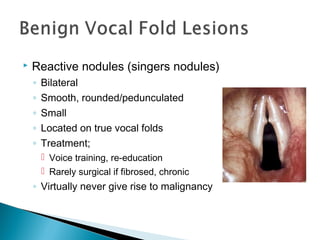




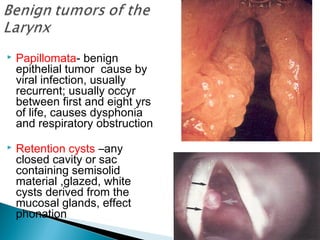
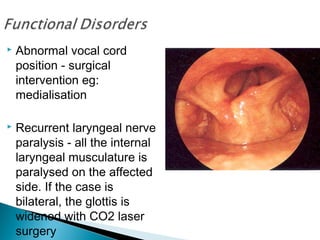


This document discusses various laryngeal conditions including laryngomalacia, laryngeal cysts, laryngeal papillomatosis, laryngeal cancer, vocal cord nodules and polyps, and various causes of laryngeal injury and paralysis. It provides descriptions of the anatomical locations, presentations, causes, and potential treatments for each condition.























































































