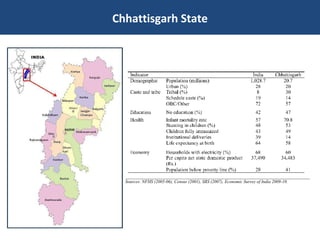
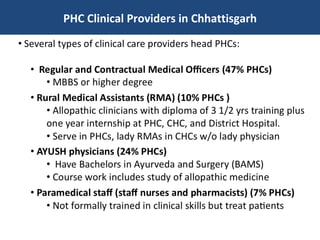
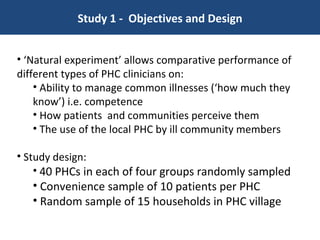
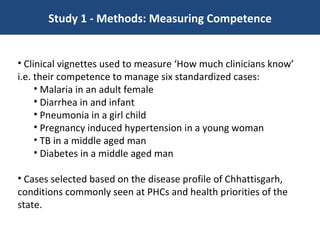
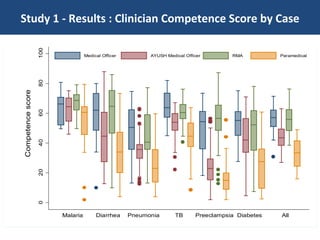
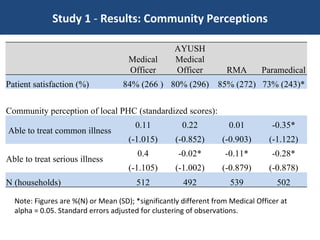
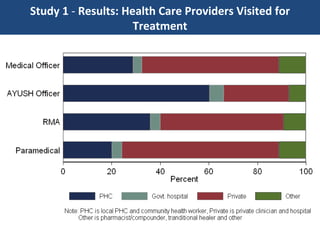
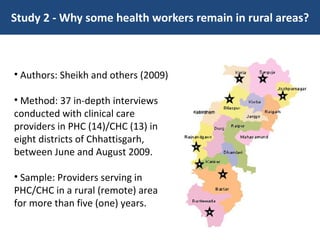
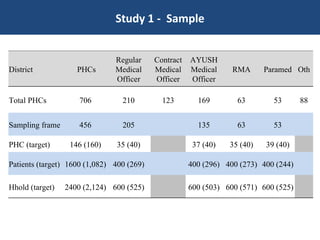
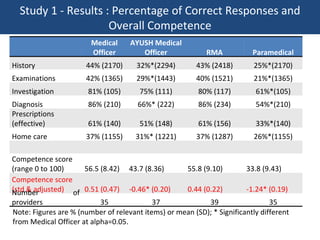
Two studies conducted in Chhattisgarh, India compared the performance of different types of primary healthcare clinicians. A natural experiment compared the competence and perceptions of Medical Officers, AYUSH Medical Officers, Rural Medical Assistants, and Paramedics. While Medical Officers scored highest on clinical vignettes, AYUSH Officers and RMAs also demonstrated competence. Communities perceived Medical Officers and RMAs as most able to treat common illnesses. A second study found that reasons such as community ties, education opportunities, and personal values motivated some clinicians to remain in rural areas long-term.













![[HOW TO] Create High Performance Emergency Departments](https://cdn.slidesharecdn.com/ss_thumbnails/edperformancewhitepaper-140110130313-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)