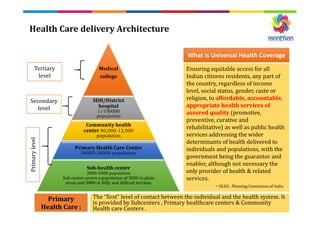
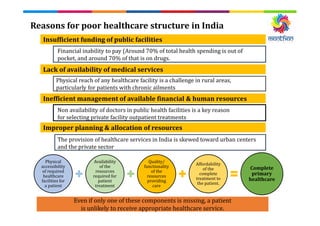
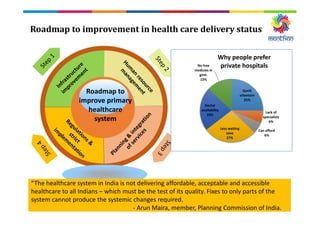
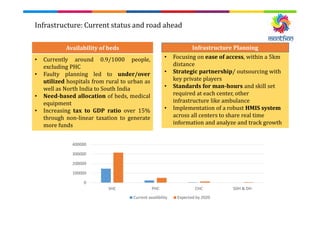
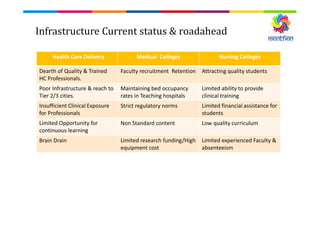
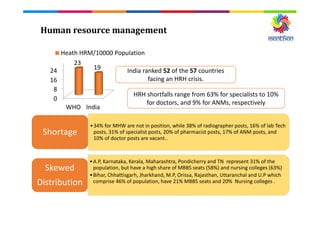
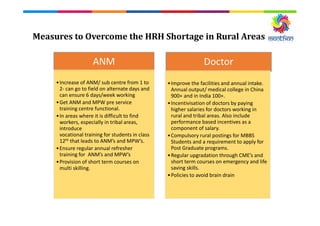
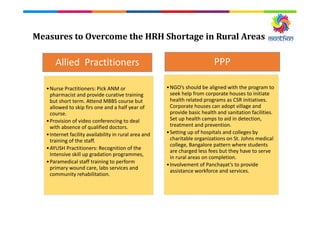
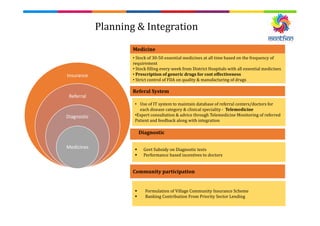
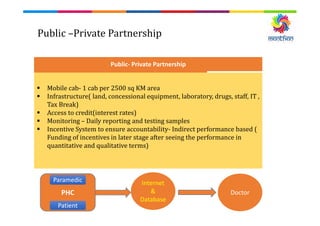
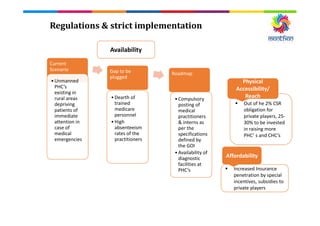
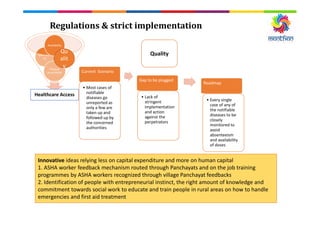
The document discusses universalizing access to primary healthcare in India. It outlines the current healthcare structure and reasons for poor access, including insufficient funding, lack of availability and affordability. It proposes a roadmap to improve the system through measures like increasing infrastructure and availability of resources, improving human resource management, strengthening regulations, and public-private partnerships. The goal is to ensure equitable, affordable and quality healthcare access for all Indians.






















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)